ABSTRACT
OBJECTIVES: to analyze the temporal trend and spatial distribution of infant mortality in Pernambuco from 2001 to 2019.
METHODS: an ecological study involving all deaths in children under one year of age living in the state. Data were collected from the Mortality Information System and the Live Birth Information System. Four mortality rates were calculated and the temporal analysis was performed by applying the regression model by inflection points of the rates at different spatial levels.
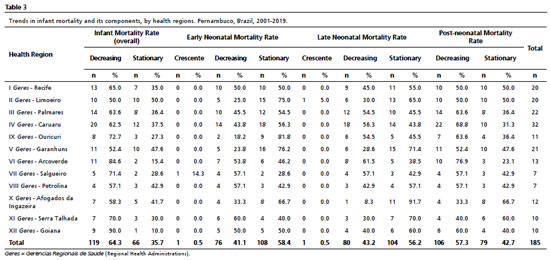
RESULTS: 47,949 deaths were recorded, of which 51.0% (n=24,447) occurred in the first six days of life. A statistically significant downward trend was observed in all the rates analyzed (-4.5%/year in overall mortality, -3.6%/year in early neonatal mortality, -1.9%/year in the late neonatal component, and -6.3%/year in the post-neonatal component). Additionally, 64.3% of the municipalities (n=119) showed a declining trend in the overall infant mortality rate. Less than 50% of the municipalities showed a downward trend in early neonatal and late neonatal mortality (41.08%; n=76 and 43.2%; n=80, respectively). In post-neonatal mortality, 57.3% (n=106) showed decreasing trends.
CONCLUSIONS: there was a temporal trend of decline in overall infant mortality, although there is an important portion of municipalities with a stationary trend, justifying the need to reduce social inequalities and geographical asymmetries.
Keywords:
Time series, Morbidity and mortality, Epidemiology
RESUMO
OBJETIVOS: analisar a tendência temporal e a distribuição espacial da mortalidade infantil em Pernambuco no período de 2001 a 2019.
MÉTODOS: estudo ecológico envolvendo todos os óbitos em crianças menores de um ano residentes no estado. Os dados foram coletados no Sistema de Informações sobre Mortalidade e no Sistema de Informação sobre Nascidos Vivos. Foram calculados quatro coeficientes de mortalidade e a análise temporal foi realizada aplicando o modelo de regressão por pontos de inflexão dos coeficientes em diferentes níveis espaciais.
RESULTADOS: foram registrados 47.949 óbitos, dos quais 51,0% (n=24.447) ocorreram nos seis primeiros dias de vida. Foi observada tendência de declínio estatisticamente significativo em todos os coeficientes analisados (-4,5%/ano na mortalidade geral, -3,6%/ano na neonatal precoce, -1,9%/ano no componente neonatal tardio e de -6,3%/ano no componente pós-neonatal). Adicionalmente, 64,3% dos municípios (n=119) apresentaram tendência de declínio no coeficiente de mortalidade infantil geral. Menos de 50% dos municípios apresentaram tendência de redução na mortalidade neonatal precoce e neonatal tardia (41,08%; n=76 e 43,2%; n=80, respectivamente). Na mortalidade pós-neonatal, 57,3% (n=106) apresentaram tendências decrescentes.
CONCLUSÕES: houve tendência temporal de declínio da mortalidade infantil geral, embora haja importante parcela de municípios com tendência estacionária, justificando a necessidade de reduzir desigualdades sociais e assimetrias geográficas.
Palavras-chave:
Série temporal, Morbimortalidade, Epidemiologia
IntroductionInfant mortality is an indicator that estimates the risk of a live birth (LB) dying before completing one year of life.
1 It is one of the most important indicators of the health situation, socioeconomic development, and quality of life of a population.
2 In this sense, high mortality rates reflect poor living and health conditions and low economic and social development, while their decrease is linked to improvements in access to health services, housing and food conditions, income distribution, and the mother's level of education.
3Globally, infant mortality has reduced from an estimated 65 deaths per 1000 LB in 1990 to 27 deaths per 1000 LB in 2020. Annual child deaths fell from 8.7 million deaths in 1990 to 3.8 million in 2020. In 2018, 75% of all under-five deaths occurred in the first year of life, totaling 4.0 million, of which 2.5 million occurred in the neonatal period.
4In Brazil, although there has been a decline in the mortality rate in all regions over the last decades, socio-spatial inequalities still persist,
5 with the highest infant mortality rates in the country's North and Northeast regions. Between 2017 and 2019, for example, these regions presented a rate of 16.9/ thousand LB and 15.3/ thousand LB respectively, values that are above the national average (13.3/ thousand LB) for the period.
3During the first year of life, the causes of infant mortality can vary. It is therefore subdivided into two segments, neonatal (0-27 days) and post-neonatal (28 days to less than one year). The neonatal period is also subdivided into early neonatal (0 to 6 days of life) and late neonatal (7 to 27 days of life).
3 Among the main causes of early neonatal mortality are prematurity, low birth weight, and bacterial sepsis of the newborn, usually associated with maternal hypertensive disorder, maternal urinary tract infections, among others. The main causes of late neonatal mortality are bacterial sepsis of the newborn, congenital malformations, and maternal conditions. In the post-neonatal period, the main causes of mortality are diarrheal diseases and gastroenteritis of presumed infectious origin, pneumonia due to unspecified microorganisms, and other septicemias.
6Since each age component has specific causes of mortality, the epidemiological monitoring of indicators over the years is fundamentally important. Among the available tools, time serial analysis stands out, a statistical tool that allows monitoring the evolution of a data set over time, which in this case is expressed in years.
7In addition, the time series makes it possible to identify non-random variations (inflections), caused, for example, by the implementation of a policy, plan, or strategy, as well as seasonality patterns or even noise, which are expressed as random facts that have modified the evolution of the data.
7 Thus, time series analysis of infant mortality is a useful tool for monitoring indicators over time, producing knowledge about temporal evolution and enabling decision-making by managers.
In a state characterized by socioeconomic disparities, such as Pernambuco, in which more than half of the municipalities are classified as very highly vulnerable, located mainly in the inner part of the state,
8 time series studies can help in understanding the different local scenarios, contributing to identifying priority areas for intervention, such as those municipalities that show a tendency to increase infant mortality.
Based on the above, this study aims to analyze the temporal trend and spatial distribution of infant mortality in Pernambuco from 2001 to 2019.
MethodsThis is an ecological study involving all deaths in children under one year of age living in the state of Pernambuco, considering from 2001 to 2019. 2020 and subsequent years were not included due to the Covid-19 pandemic. Considering the impacts of Covid-19, it is likely that they would influence the time trend. Thus, this is a pre-Covid-19 pandemic study.
The state of Pernambuco is located in the Northeast region of Brazil and is composed of 185 municipalities. The state's population was estimated to be 9.6 million in 2020, making it the seventh most populous in the country.
8 For health purposes, the state is subdivided into 12 health regions that take into account care flows, health networks, and neighboring municipalities.
For this study, four mortality rates were analyzed, namely (1) overall infant mortality / 1,000 LB; (2) early neonatal mortality / 1,000 LB; (3) late neonatal mortality / 1,000 LB, and (4) post-neonatal mortality / 1,000 LB, whose equations for calculation are represented below:
9 The raw data needed to calculate the indicators were from the Mortality Information System (MIS) and the Live Birth Information System (SINASC -
Sistema de Informação sobre Nascidos Vivos), which are available on the Department of Informatics of the Unified Health System platform. The MIS, developed by the Ministry of Health in 1975, provides information that enables the creation of indicators and the organization of epidemiological analyses to contribute to health management.
10 SINASC, implemented in 1990, aims to collect data on births registered in the national territory and, thus, provide birth data,
10 both have national coverage.
The joinpoint regression model of the four rates at the different spatial levels (state, health regions, and municipalities) was used to perform the temporal analysis. This model tests whether a line with multiple segments is statistically better to describe the temporal evolution of the data than a straight line or one with fewer segments.
11 Thus, the model allows identifying the indicator's temporal behavior (whether stationary, increasing, or decreasing) through the slope of the regression line, the points where there is a change in this trend (joins), the Annual Percentage Change (APC) and the average variation of each period (AAPC- Average Annual Percent Change).
12 Parameters used in the joinpoint analysis: minimum: 0; maximum: 4; model selection: test with 4,499 permutations, 5% significance, 95% confidence interval and autocorrelation of errors based on date.
The analyses were performed using the Joinpoint Regression software, version 4.5.0.1 (National Cancer Institute - USA). Additionally, choropleth maps were prepared for the presentation of the results using QGIS 2.14.11 (Open Source Geospatial Foundation OSGeo). The territorial meshes necessary for making the maps were obtained from the Brazilian Institute of Geography and Statistics (IBGE -
Instituto Brasileiro de Geografia e Estatística).
ResultsFrom 2001 to 2019, 47,949 infant deaths under one year of age were recorded in the state of Pernambuco. Of these, 51.0% (n=24,447) occurred in the first six days of life (early neonatal period), 13.7% (n=6,569) between the seventh and twenty-seventh day (late neonatal period), and 35.3% (n=16,907) after the twenty-seventh day (post-neonatal period).
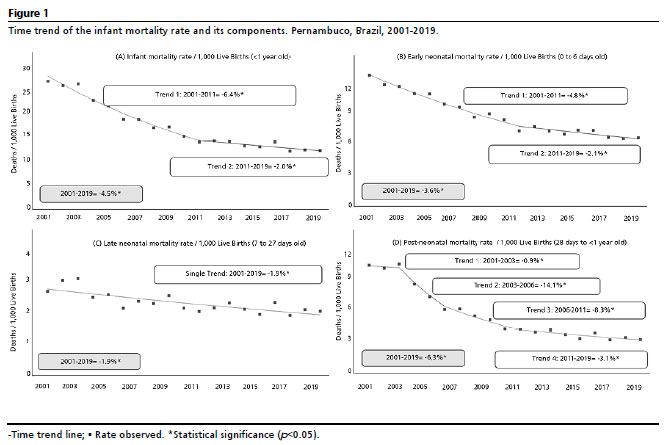
At the beginning of the time series (2001), the infant mortality rate in Pernambuco was 26.6/thousand LB. A more intense decline was observed from 2001 to 2011 (-6.4% per year), from which the annual reduction became -2.0% per year, reaching a rate of 17.5/1,000 LB in 2019. The late neonatal component decreased the least (-1.9% per year). On the other hand, post-neonatal mortality showed more variations over the time series (three junctions and four trends), and with an average percentage reduction of -6.3% per year (from 12.8/1,000 LB in 2001 to 8.9/1,000 LB in 2019) (Figure 1).
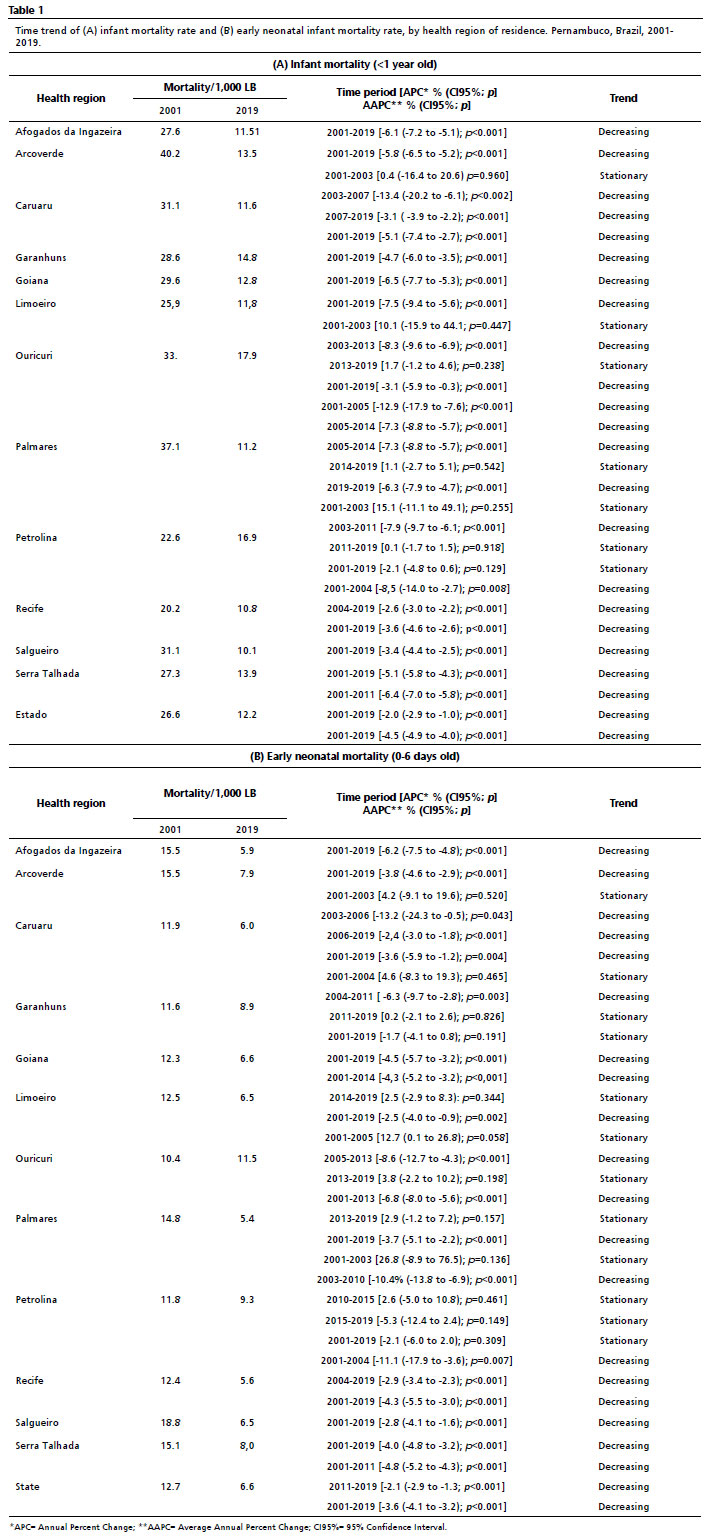
Only the Petrolina region (in the state's outback) showed stationary temporal behavior in the overall infant mortality rate (AAPC=-2.1;
p=0.129) between 2001 and 2019. On the other hand, in the health region of Limoeiro, the greatest decline was recorded (AAPC=-7.5%;
p<0.001), whose rate went from 25. 9/1,000LB in 2001 to 11.8/1,000 LB in 2019. In addition, six of the twelve health regions had higher mortality rates than the state in the 2001-2019 time series, with emphasis on the two regions of the Pernambuco outback that ranked first: Ouricuri (17.9/1,000 LB) and Petrolina (16.9/1,000 LB) (Table 1A).
As for early neonatal mortality, nine regions showed a declining trend, with Afogados da Ingazeira standing out (AAPC=-6.2%;
p<0.001). There, the early neonatal mortality rate decreased from 15.5/1,000 LB to 5.9/1,000 LB. In addition, six of the twelve health regions had higher mortality rates than the state, especially Ouricuri and Petrolina, which occupied the first positions (11.5/1,000 LB and 9.3/1,000 LB, respectively) (Table 1B).
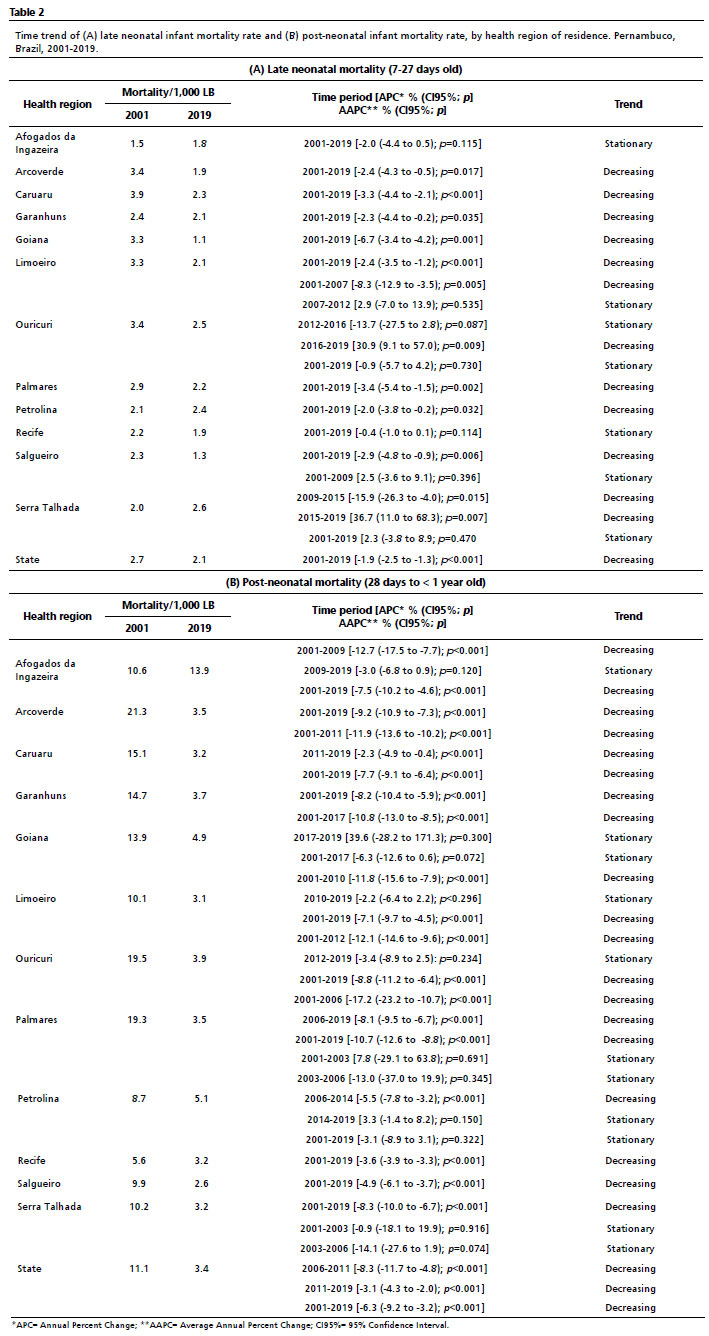
Late neonatal mortality was the lowest among the rates. In this component, with the exception of the regions of Afogados da Ingazeira, Ouricuri, Recife, and Serra Talhada, in which the temporal trend was stationary, all the others showed decreasing trends: Goiana was the region with the highest decline in percentage between 2001 and 2019 (-6.7% per year), with a reduction from 3.3/1,000 LB to 1.1/1,000 LB. Six of the twelve health regions had higher mortality rates than the state in the time series (2001-2019), with Serra Talhada (2.6/1,000 LB), Ouricuri (2.5/1,000 LB), and Petrolina (2.4/1,000 LB) occupying the first positions (Table 2A).
In the post-neonatal component, ten municipalities showed a decline in the period 2001-2019, with the municipalities of Palmares (AAPC=-10.7%;
p<0.001), Arcoverde (AAPC=-9.2;
p<0.001) and Serra Talhada (AAPC= -8.3;
p<0.001) standing out. In Palmares, for example, the rate decreased from 19.3/thousand LB to 3.5/ thousand LB. In addition, seven of the twelve health regions had mortality rates higher than the state rate, especially the Afogados da Ingazeira area, whose mortality in 2019 was 4.08 times higher than the state rate (13.9/1,000 LB and 3.4/1,000 LB), respectively (Table 2B).
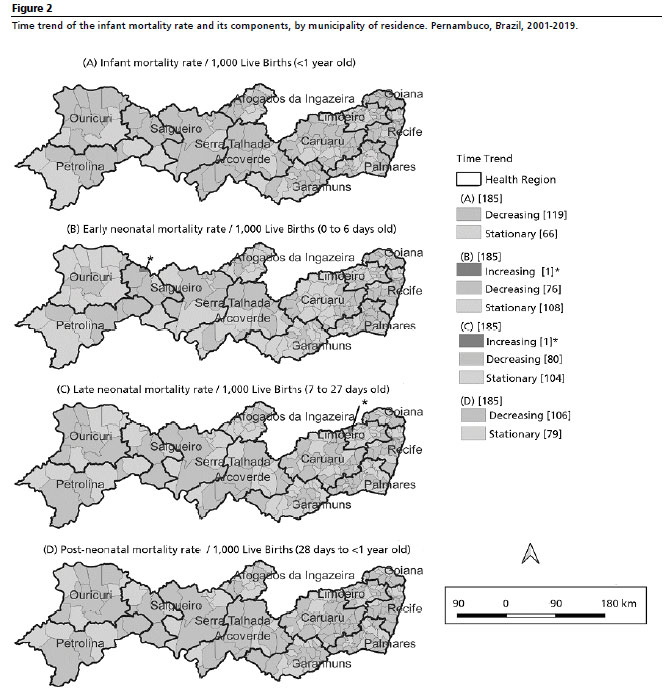
In the municipal analysis, 64.3% of the municipalities (n=119) showed a declining trend in the overall infant mortality rate. Less than 50% of the municipalities showed a downward trend in early neonatal and late neonatal mortality (41.08%; n=76 and 43.2%; n=80, respectively). Increasing trends in early neonatal mortality were observed in the municipality of Cedro (AAPC=58.9%;
p<0.001) and in late neonatal mortality in Casinhas (AAPC=29.5%;
p=0.012). Finally, in post-neonatal mortality, 57.3% (n=106) showed decreasing trends (Figure 2).
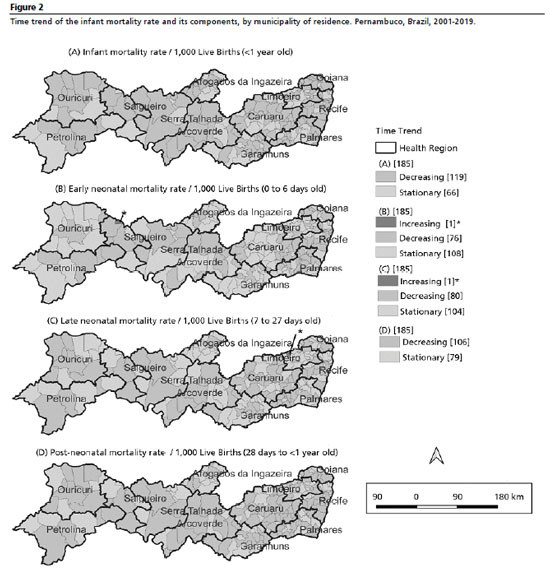
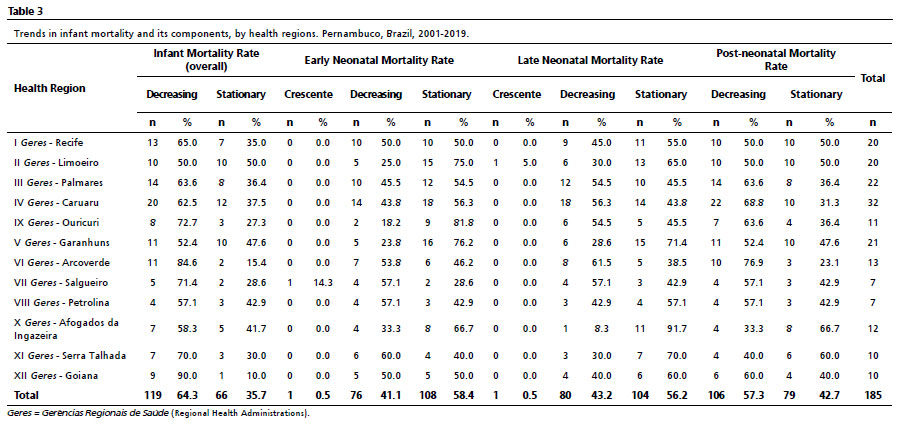
When entering the municipalities of each health region, Goiana had the highest proportion of municipalities with a decreasing trend (90%; n=9) in the overall infant mortality rate, while only half of the municipalities in the Limoeiro region showed a declining trend. In the early neonatal component, the Serra Talhada region showed the highest proportion of municipalities with a decreasing trend (60%; n=6), and the Ouricuri region the lowest (18.2%; only two of the eleven municipalities). In late neonatal mortality, the region of Arcoverde occupied the best position (61.5% of municipalities showed a declining trend), and the region of Afogados da Ingazeira the worst (only one of the twelve municipalities showed a declining trend). Finally, in post-neonatal mortality, the best position was occupied by the Caruaru region, in which 68.8% (n=22) of the municipalities showed a declining trend, while the Afogados da Ingazeira health region had the lowest proportion of municipalities with a declining trend (33.3%; n=4) (Table 3).
This study analyzed the temporal trend of Infant Mortality in Pernambuco from 2001 to 2019, showing that there was a more intense decline in overall infant mortality until 2011, with a greater number of inflections in post-neonatal mortality. Regional differences in the time trend were also observed, with just over half of the municipalities showing a significant decline in the overall infant mortality rate.
As seen in Brazil, the state of Pernambuco has shown a reduction in infant mortality and its components.
3 Overall infant mortality is an important indicator of the population's living conditions and the decrease in values of this indicator is related to the decrease in social inequality and improved access to and supply of health services since there is a direct correlation between these variables.
11,13Therefore, there is a consensus in the scientific literature that a significant proportion of deaths are preventable, that is, these are deaths that derive from health inequities, i.e. , unfair social inequalities, such as poor access to health services and family living conditions (education, housing, and income).
11 These deaths can be prevented, partially or totally, with the implementation of public policies, plans, or strategies aimed at social determinants.
14Addressing infant mortality is still one of the greatest challenges for a country's development, given the problem's complexity and, thus, demands cross-cutting and integrated policies to act on its social determinants.
14 In this scenario, studies point out, for example, that the decline in infant mortality is related to social programs implemented in Brazil in recent decades, such as the
Bolsa Família Program (PBF), created in 2003.
15,16An ecological study conducted in Brazil to assess the impact of the PBF on deaths in children under five years of age showed that the cash transfer program is able to contribute to the reduction of overall child mortality, in particular for deaths attributable to poverty-related causes such as malnutrition and diarrheal diseases.
15 Bolsa Família is an income transfer program that benefits families in poverty or extreme poverty, acting to reduce, above all, deaths in the post-neonatal period.
17 In Pernambuco, a study showed that
Bolsa Família improved the quality of individuals' diets benefiting from the program, with an increase in the variety of foods consumed, for example.
18In addition to income transfer policies, specific programs have been created for maternal and child health, such as the
Mãe Coruja Program, which operates through intersectoral and health actions aimed at pregnant women during prenatal care, childbirth and postpartum, and children up to the fifth year of life.
13 However, in a study aimed at analyzing the impact of
Mãe Coruja on the reduction of infant mortality in Pernambuco, it was shown that there was no direct relationship between the beginning of infant mortality decline and the implementation of the program, demonstrating that other factors may be associated with the reduction of mortality.
13Even with the benefits brought by these policies, only 64.3% of the municipalities in Pernambuco showed a declining trend in the overall infant mortality rate. It is worth noting that Petrolina was the only region with a stationary pattern, in the region of Petrolina, of the seven municipalities that make it up, all are part of the
Mãe Coruja program and three showed a stationary pattern (Afrânio, Petrolina, and Cabrobó). These findings reinforce what has already been pointed out by the scientific literature regarding this program, which alone is not able to reduce preventable deaths to minimum acceptable levels.
13 In addition, each region has its own singularities, which signals the need for public policies that take into account this particular condition.
Primary Health Care (PHC) has also been identified as an important mechanism capable of reducing infant mortality. Materialized through the Family Health Strategy (FHS), PHC has allowed the population to have greater access to services aimed at maternal and child health, characterizing an advance in the quality of care provided.
19,20 An ecological study conducted in Brazil between 1999 and 2004 verified that increasing FHS coverage by 10% led to a 0.45% decrease in the infant mortality rate, 0.6% of which was in the post-neonatal component.
21However, other studies have shown that the PHC alone also had no impact on infant mortality, so it is not possible to attribute sole responsibility for the observed decrease to this component of the health system over the time series.
22 An investigation carried out in Garanhuns, in the
agreste (is hillynarrow zone of Brazil in the states of Rio Grande do Norte, Paraiba, Pernambuco, Alagoas, Sergipe, and Bahia) of the state of Pernambuco, when comparing the trend of infant mortality between areas covered and not covered by the PHC, found no correlation between these variables.
22In this regard, it seems increasingly evident that addressing infant mortality requires a collective effort on different fronts, which go far beyond the health system but must reach the population's living conditions. An investigation conducted in Recife showed that, as living conditions worsened, the infant, neonatal and post-neonatal mortality rates increased.
23 It is not only the income variable, but a whole chain of social determinants that, by nature, is dynamic, polysemic, and multifaceted.
In addition to regional differences and the complexity surrounding the issue, it is necessary to consider a third dimension of the phenomenon - the components of infant mortality. The neonatal component has presented itself as a greater challenge than that of post-neonatal mortality, since the latter is more susceptible to overall improvements in people's living conditions and to health sector interventions, such as preventive vaccination and breastfeeding strategies, for example.
2,24 In this study, 57.3% of the municipalities showed a declining trend in the post-neonatal component and, from the regional point of view, Goiana and Petrolina had a stationary pattern, while there was a more intense decline in the regions of Palmares, Arcoverde and Serra Talhada.
Different investigations have already shown a higher number of deaths in the early neonatal period.
25,26 Conditions such as prematurity and low birth weight have been associated with this mortality, which are avoidable and can be identified and prevented during prenatal care. In general, these conditions are secondary to other conditions, such as hypertensive disease, maternal urinary tract infections, and cervical dysfunction, for example.
27 In this regard, the role of PHC is emphasized through the promotion of actions that directly influence these vital statistics, such as family planning, prenatal care, vaccination coverage, breastfeeding counseling, and neonatal visits in the first week of life.
22Regarding late neonatal mortality, the two main causes of death reported by data from the Ministry of Health were newborn bacterial septicemia and newborn respiratory distress, between 2001 and 2019.
6 In this study, this rate is the lowest and, except for the municipality of Casinhas, no other showed an upward trend.
Deaths from septicemia in the late neonatal period may be related to several post-birth scenarios, such as the various hospital invasive procedures, horizontal transmission of infections by the hands of caregivers (home or hospital care team), in addition to inadequate post-birth follow-up by the PHC team. On the other hand, deaths due to respiratory distress may be related to the care provided in the delivery room and in the Neonatal Intensive Care Unit (NICU), the absence of such a unit in the municipality being a complicating factor.
28,29Even considering the methodological care taken, this study has limitations. The first concerns the use of secondary data, which are subject to the influence of the health surveillance systems of the municipalities. It is well-known that in smaller municipalities death surveillance faces even greater challenges, especially with regard to the ability to investigate deaths and monitor the quality of records. On the other hand, mortality records are considered the most reliable among information systems.
Finally, this study showed a temporal trend of decline in overall infant mortality in Pernambuco from 2001 to 2019, despite the existence of intraregional differences, with an important share of municipalities with a stationary trend in infant mortality. Such differences justify the need for sociopolitical efforts in an attempt to reduce existing social inequalities and geographical asymmetries, in addition to reinforcing the need to address preventable infant and under-one-year deaths.
References1. OECD/World Health Organization. Infant mortality. In: OECD/World Health Organization. Health at a Glance: Asia/Pacific 2020: Measuring Progress Towards Universal Health Coverage. Paris: OECD Publishing; 2020. p. 44-6. [access in 2023 Feb 8]. Available from:
https://www.oecd-ilibrary.org/social-issues-migration-health/health-at-a-glance-asia-pacific-2020_26b007cd-en2. Souza CDF, Albuquerque AR, Cunha EJO, Silva Junior LCF, Silva JVM, Santos FGB, et al. Novo século, velho problema: tendência da mortalidade infantil e seus componentes no Nordeste brasileiro. Cad Saúde Colet. 2021; 29 (1): 133-42.
3. Ministério da Saúde (BR). Mortalidade infantil no Brasil. Boletim Epidemiológico. 2021; 52 (37): 1-15. [access in 2023 Feb 8]. Available from:
https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/edicoes/2021/boletim_epidemiologico_svs_37_v2.pdf4. World Health Organization (WHO). The Global Health Observatory. Indicators [Internet]. Genebra: WHO; 2023 [access in 2023 Feb 8]. Available from:
https://www.who.int/data/gho/data/indicators5. Alves FJO, Ramos D, Paixão ES, Falcão IR, Ribeiro-Silva RC, Fiaccone R, et al. Association of Conditional Cash Transfers With Maternal Mortality Using the 100 Million Brazilian Cohort. JAMA Netw Open. 2023 Feb; 6 (2): e230070.
6. Brasil. Departamento de Informática do Sistema Único de Saúde (DATASUS). Mortalidade - desde 1996 pela CID-10 - DATASUS [Internet]. Brasília (DF); 2022 [access in 2022 Nov 15]. Available from:
https://datasus.saude.gov.br/mortalidade-desde-1996-pela-cid-10/7. Antunes JL, Cardoso MRA. Uso da análise de séries temporais em estudos epidemiológicos. Epidemiol Serv Saúde. 2015; 24 (3): 565-76.
8. Julião CCB, Lima JE. Índice de vulnerabilidade social: uma aplicação de análise fatorial para classificar os municípios pernambucanos. Planej Polít Públicas. 2020; 54: 11-28.
9. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Secretaria de Atenção à Saúde. Manual de Vigilância do Óbito Infantil e Fetal e do Comitê de Prevenção do Óbito Infantil e Fetal. Brasília (DF): Ministério da Saúde; 2009. 2nd ed. [access in 2022 Nov 15]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/manual_obito_infantil_fetal_2ed.pdf10. Ministério da Saúde (BR). Portaria nº 116, de 11 de fevereiro de 2009. Regulamenta a coleta de dados, fluxo e periodicidade de envio das informações sobre óbitos e nascidos vivos para os Sistemas de Informações em Saúde sob gestão da Secretaria de Vigilância em Saúde. Brasília (DF): DOU; 2009. [access in 2022 Nov 15]. Available from:
https://bvsms.saude.gov.br/bvs/saudelegis/svs/2009/prt0116_11_02_2009.html11. Carvalho RAS, Santos VS, Melo CM, Gurgel RQ, Oliveira CCC. Inequalities in health: living conditions and infant mortality in Northeastern Brazil. Rev Saúde Pública. 2015; 49: 5
12. Kim H, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Statist Med. 2000 Feb; 19 (3): 335-51.
13. Lima SS, Braga MC, Vanderlei LCM, Luna CF, Frias PG. Avaliação do impacto de programas de assistência pré-natal, parto e ao recém-nascido nas mortes neonatais evitáveis em Pernambuco, Brasil: estudo de adequação. Cad Saúde Pública. 2020; 36 (2): 1-12.
14. Malta DC, Duarte EC. Causas de mortes evitáveis por ações efetivas dos serviços de saúde: uma revisão da literatura. Ciênc Saúde Colet. 2007; 12 (3): 765-76.
15. Cooper JE, Benmarhnia T, Koski A, King NB. Cash transfer programs have differential effects on health: a review of the literature from low and middle-income countries. Soc Sci Med. 2020; 247: 112806.
16. Duarte GB, Sampaio B, Sampaio Y. Programa Bolsa Família: impacto das transferências sobre os gastos com alimentos em famílias rurais. Rev Econ Sociol Rural. 2009; 47 (4): 903-18.
17. Souza BFN, Sousa NFC, Sette GCS, Lima APE, Leal LP, Holanda ER. Determinantes da mortalidade neonatal em município da Mata Pernambucana. Rev Esc Enferm USP. 2021; 55: e03726.
18. Coelho PL, Melo ASSA. Impacto do Programa "Bolsa Família" sobre a qualidade da dieta das famílias de Pernambuco no Brasil. Ciênc Saúde Colet. 2017 Feb; 22 (2): 393-402.
19. Lourenço EC, Guerra LM, Tuon RA, Silva SMCV, Ambrosano GMB, Corrente JE, et al. Variáveis de impacto na queda da mortalidade infantil no Estado de São Paulo, Brasil, no período de 1998 a 2008. Ciênc Saúde Colet. 2014; 19 (7): 2055-62.
20. Hatisuka MF de B, Moreira RC, Cabrera MAS. Relação entre a avaliação de desempenho da atenção básica e a mortalidade infantil no Brasil. Ciênc Saúde Colet. 2021; 26 (9): 4341-50.
21. Macinko J, Souza MFM, Guanais FC, Simões CCS. Going to scale with community-based primary care: An analysis of the family health program and infant mortality in Brazil, 1999 - 2004. Soc Sci Med. 2007; 65 (10): 2070-80.
22. Roncalli AG, Lima KC. Impacto do Programa Saúde da Família sobre indicadores de saúde da criança em municípios de grande porte da região Nordeste do Brasil. Ciênc Saúde Colet. 2006 Jul; 11 (3): 713-24.
23. Duarte EMS, Alencar ÉTS, Fonseca LGA, Silva SM, Machado MF, Araújo MDP, et al. Maternal mortality and social vulnerability in a Northeast State in Brazil: a spatial-temporal approach. Rev Bras Saúde Mater Infant. 2020; 20 (2): 575-86.
24. Falcão IR, Ribeiro-Silva RC, Alves FJO, Ortelan N, Silva NJ, Fiaccone RL, et al. Evaluating the effect of Bolsa Familia, Brazil's conditional cash transfer programme, on maternal and child health: a study protocol. PLoS One. 2022 May; 17 (5): e0268500.
25. Lima JC, Mingarelli AM, Segri NJ, Zavala AAZ, Takano OA. Estudo de base populacional sobre mortalidade infantil. Ciên Saúde Colet. 2017; 22 (3): 931-9.
26. Oliveira MND, Camargo BA, Pinto Junior EP, Luz LA. Características de óbitos infantis em um município de médio porte da região Nordeste do Brasil. J Health Biol Sci. 2017; 5 (2): 160-4.
27. Cavalcante ANM, Araújo MAL, Lopes SVS, Almeida TÍF, Almeida RLF. Epidemiologia da mortalidade neonatal no Ceará no período de 2005-2015. Rev Bras Promoç Saúde. 2018; 31 (4): 1-8.
28. Justino DCP, Lopes M, Machado FC, Andrade FB. Avaliação das causas de morbidade e mortalidade infantil no Brasil. Mundo Saúde. 2021; 45: 152-61.
29. Oliveira EAR, Lima CSO, Cirino IP, Vera PVS, Lima LHO, Conde WL. Mortalidade neonatal: causas e fatores associados. Saúde Redes. 2020; 6 (3): 113-27.
Received on April 4, 2023
Final version presented on June 26, 2023
Approved on July 6, 2023
Associated Editor: Lygia Vanderlei
Authors' contribution: Coelho LMS, Ferreira ACF, Vasconcelos RA, Matos TS and Souza CDF: study design and planning, data analysis and interpretation, drafting, and critical revision of the content. All authors have approved the final version of the article and declare no conflict of interest.


 ; Ana Carolina Furtado Ferreira2
; Ana Carolina Furtado Ferreira2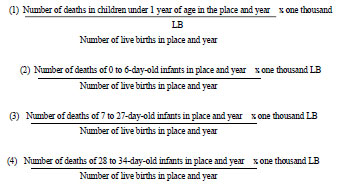






 Ler em português
Ler em português