ABSTRACT
OBJETIVOS: explorar um conjunto de fatores associados ao menor apego materno-fetal (AMF) em gestantes.
MÉTODOS: trata-se de um estudo transversal, correspondente à segunda fase de um estudo de coorte com uma amostra de base populacional de gestantes no sul do Brasil. Foi utilizada a Escala de Apego Materno-Fetal (EAMF) para medir o AMF. A análise bivariada foi realizada através do teste t e ANOVA. As variáveis que apresentaram p<0,20 foram levadas para análise multivariada, por meio de regressão linear, a fim de controlar possíveis fatores de confusão.
RESULTADOS: foram incluídas 840 gestantes. As gestantes que apresentaram menores médias de AMF foram aquelas que não moravam com um companheiro (B=-3,8 [IC95%=-6,0; -1,7]), que estavam entre o primeiro e o segundo trimestre de gestação (B=-4,3 [IC95%=-5,9; -2,6]), que não tiveram o apoio da mãe durante a gestação (B=-2,4 [IC95%=-4,6; -0,2]) e que apresentaram sintomas depressivos (B=-4,9 [IC95%=-7,4; -2,5]).
CONCLUSÕES: os resultados mostraram que um maior AMF está associado a presença de uma rede de apoio adequada na gravidez, melhor saúde mental materna e a uma gestação avançada. A avaliação precoce do AMF e a promoção de um vínculo pré-natal adequado, com foco nos aspectos psicológicos e emocionais maternos são fortemente sugeridos.
Keywords:
Apego materno-fetal, Vínculo pré-natal, Apoio social, Saúde materna, Gravidez
RESUMO
OBJECTIVES: this study aimed to explore a set of factors associated with lower maternal-fetal attachment (MFA) in pregnant women.
METHODS: this is a cross-sectional study corresponding to the second wave of a cohort study with a population-based sample of pregnant women in the South of Brazil. The maternal-fetal attachment scale (MFAS) was used to measure MFA. Bivariate analysis was performed using the t-test and ANOVA. The variables that presented p<0.20 were taken for multivariate analysis, through linear regression, in order to control possible confounding factors.
RESULTS: a total of 840 pregnant women were included. Pregnant women who had lower MFA means were those who did not live with a partner (B=-3.8 [CI95%=-6.0; -1.7]), those between the first and second trimester of pregnancy (B=-4.3 [CI95%=-5.9; -2.6]), those who did not have support from their mother during pregnancy (B=-2.4 [CI95%=-4.6; -0.2]), and those with depressive symptoms (B=-4.9 [CI95%=-7.4; -2.5]).
CONCLUSIONS: the results showed that a higher MFA it is associated with an adequate support network during pregnancy, better maternal mental health, and with an advanced pregnancy. Early evaluation of MFA and effort to promote an adequate prenatal bond, focusing on maternal psychological and emotional aspects are strongly suggested.
Palavras-chave:
Maternal-fetal attachment, Prenatal bonding, Social support, Maternal health, Pregnancy
IntroductionThe transition into the mother's role involves not only physical, psychological, and social changes in a woman's life, but also a change in habits in favor of maternal-fetal health to build a bond with the child.
1 According to Dipietro
2 studies that originated in the 1960's sparked a great empirical interest in the prenatal period and the influence of maternal aspects on pregnancy and children's later development. In this context, attachment, which was previously seen as an infant's innate tendency to establish emotional bonds, especially with the maternal figure, in the first year of life, is now considered a phenomenon that has its origins even in the prenatal period.
3Maternal-fetal attachment (MFA) refers to the emotional bonding between a mother and her unborn child during pregnancy. This bond can be seen as the mother's expectations, thoughts, emotions, and behaviors regarding her fetus, motherhood, and pregnancy.
4 Cranley
5 described MFA as the extent to which women engage in behaviors that represent affiliation and interaction with their expected child.
Previous studies have shown how different psychosocial and socio-demographic characteristics report prenatal bonding. Factors such as lower gestational age, lack of social support during pregnancy, and the presence of maternal psychiatric disorders, including anxiety and depression, are often associated with low levels of MFA.
6-9 However, a national study showed that the MFA was not associated with anxiety or depression, but included only pregnant women diagnosed with congenital malformations, which limits the comparison of data with other samples.
10A literature review by Cannella
11 demonstrated that lower economic and schooling levels and higher maternal age were associated with lower MFA scores. However, most studies have not found this relationship.
7,12 According to Kelmanson
12 overall, demographic factors like age, marital status, income, parity, education, and ethnicity do not appear to considerably impact MFA. Moreover, some risky behaviors during pregnancy, such as tobacco and alcohol use, are frequently observed in pregnant women with low levels of MFA and can have negative effects on the fetus' health and cause developmental delay after birth.
13-15 On the other hand, other studies have focused on positive factors, such as social support, support from the partner, or from the pregnant woman's parents, that have been related to a more positive prenatal bonding.
8,16It is noteworthy that studies where both supportive and risk factors are explored together are rare, especially in least developed countries, such as Brazil. According to Foley
17 studies are increasingly recognizing the importance of pregnancy as a period of potential risk and opportunity for intervention. However, the authors indicated that few studies on maternal psychological health have been conducted in least developed countries. Thus, to explore factors that can serve as protection for pregnancy and child's outcomes is appropriate. Mainly because MFA can serve as a useful indicator for an early clinical and psychological intervention in this population.
12Despite of a growing body of evidence regarding MFA, few studies have rigorous methodology, population-based samples, and validated instruments, leading the findings in the literature to be inconsistent. Thus, given the evidence that demonstrates the influence of MFA on the offspring's outcomes, it is important to identify the factors that are related to lower MFA, so that early interventions can be implemented during pregnancy in order to reduce maternal and child impairment. To address the issue and bridge the gap, the aim of this study was to explore a set of maternal factors associated with MFA in a sample of pregnant women in the South of Brazil.
MethodsThis is a cross-sectional study corresponding to the second wave of a population-based cohort of pregnant women living in a city in the South of Brazil. The city is medium-sized, with approximately 330.000 inhabitants. According to the 2010
Instituto Brasileiro de Geografia e Estatística (Census of the Brazilian Institute of Geography and Statistics), the urban zone of Pelotas contains 488 census sectors. Out of these, 244 (50%) were randomly drawn to search for pregnant women up to the second trimester. The inclusion criteria were determined as follows: women up to 24 weeks of pregnancy and living in the urban area of the city. Pregnant women who were unable to respond to and/or understand the research tools due to physical and/or cognitive problems were excluded from the study.
1072 pregnant women were identified. However, 91 (8.5%) had lost the baby before the first evaluation or refused to participate in the study, the remaining 981 (91.5%) pregnant women were evaluated in the first evaluation. Of these, 14.4% were considered losses or refusals, or they lost the baby before the second evaluation. Thus, the total sample of this study consisted of 840 (85.6%) pregnant women, who participated in the first and second evaluations. Data were collected through printed questionnaires, administered by trained interviewers. Home interviews were held in the first wave of the study. Meanwhile, in the second wave, the interviews occurred in a room at the university hospital.
MFA was assessed using the Maternal-Fetal Attachment Scale (MFAS). This scale is a 24-item measure that contains 5-point Likert-type items with options of response ranging from 1 (definitely no) to 5 (definitely yes). Examples of MFAS items include "I talk to my unborn child" and "I do things to try to stay healthy that I would not do if I were not pregnant". The total score ranges from 24 to 120.
5 In the validation process for the Brazilian population,
3 suggested that the MFA construct is one-dimensional and therefore should be used as a general measurement for bonding. Higher scores indicate higher levels of MFA. It presented a low reliability for the Brazilian context, with a Cronbach's α of 0.63.
3 However, a previous study carried out with the same sample as the present study showed an α of 0.82, indicating good reliability.
18 This instrument was used in the second wave of the study.
Depressive symptoms during gestation were evaluated using the Edinburgh Postnatal Depression Scale (EPDS). This 10 item self-report measurement is designed to screen women for symptoms of emotional distress during pregnancy and the postnatal period. Each item is scored from 0 to 3 and the total score ranges from 0 to 30. Higher scores indicate major depressive symptoms. In this study, the cutoff point used was 11. Those participants who presented 0-10 points were absent or had minor symptoms and those with 11 points or more exhibited depressive symptoms (no/yes, respectively).
19 It presented a good reliability for the Brazilian context, with a Cronbach's α of 0.87.
20 This instrument was used in the second wave of the study.
The Beck Anxiety Inventory (BAI) was used to evaluate anxiety symptoms during gestation. This is a self-administered instrument composed of 21 items that is used for measuring the severity of anxiety. Respondents were asked to rate each item on a 4-point scale ranging from 0 (not at all) to 3 (severely, can barely stand it). Ratings are for the past week. Items are summed to obtain total scores ranging from 0 to 63. Higher scores indicate greater severity of anxiety symptoms. In this study, the results were dichotomized (yes/no). Pregnant women who scored 11 points or more presented anxiety symptoms.
20 It presented a good reliability for the Brazilian context, with a Cronbach's α of 0.88-0.92.
21 This instrument was used in the second wave of the study.
In this study, the modules of the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) were applied and covers dependent use of alcohol and tobacco. ASSIST is a questionnaire that screens for all levels of problem or risky use of substance in adults. It consists of eight questions covering tobacco, alcohol, cannabis, cocaine, amphetamine-type stimulants, inhalants, sedatives, hallucinogens, opioids and 'other drugs'. Each answer corresponds to a score ranging from 0 to 4, with the total of score ranging from 0 to 20. The score ranging from 0 to 3 indicated occasional use of alcohol and tobacco, 4 to 15 revealed abuse, and ≥16 as suggestive of dependence. For this study, we grouped the categories of abuse and dependence. Thus, the classification of occasional use and abuse/dependence was considered. The reliability of the instrument for the Brazilian context was good, with a Cronbach's α of 0.80 for both alcohol and tobacco.
22 This instrument was used in the first wave of the study.
The socio-economic status of the participants was evaluated using the classification proposed by the
Associação Brasileira de Empresas de Pesquisas (ABEP) (Brazilian Association of Research Companies). This classification is based on the total accumulated material assets of the family and the householder's schooling. The individuals are categorized into five economic levels from A (highest socioeconomic status) to E (lowest socioeconomic status). In this study, "A+B" refers to the highest economic level, "C" to middle class, and "D+E" to the lowest.
23A self-report questionnaire was also applied and included variables such as: schooling in years of studying (up to 3 years, 4 to 7 years, 8 to 10 years, 11 years or more), age (up to 23, 24 to 29 years, above 30 years), living with a partner (no, yes), trimester of pregnancy (first and second trimester, third trimester), previous pregnancy (no, yes), planned pregnancy (no, yes), mother's support (no, yes) and child's father support (no, yes).
Descriptive analysis of data was performed by calculating absolute and relative frequencies and means and standard deviations. Bivariate analysis was performed using the t-test and ANOVA to verify differences in the means. In the multiple regression, the raw and adjusted analyses were performed using Linear Regression. The variables that presented
p<0.20 in the crude analysis were included in the adjusted analysis. The adjusted analysis was performed with the objective of controlling possible confounding factors and followed a conceptual hierarchical model. This model is divided into levels and assumes that variables located at the hierarchically higher level are determinants of the lower levels. Thus, the variables were controlled using the same or previous levels. Only the variables with
p-values <0.05 remained in the models.
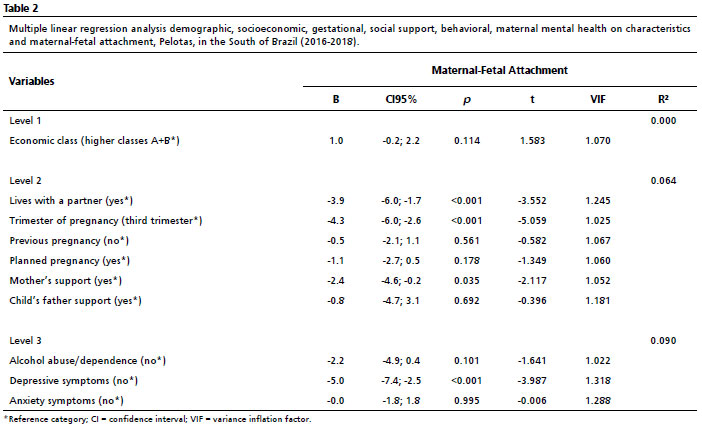
The model proposed for the approach of variables was determined in three levels. Level 1 included economic class. Level 2 included lives with a partner, trimester of pregnancy, previous pregnancy, planned pregnancy, mother's support and child's father support. Level 3 included alcohol abuse/dependence, depressive symptoms and anxiety symptoms.
P-values <0.05 were considered to indicate statistical significance.
To verify the multicollinearity in the regression analyses between the variables that remained in the regression model, we calculated the variance inflation factor (VIF). We considered values above 0.4 as the existence of collinearity among the variables. All statistical analyses were conducted using the Statistical Package for the Social Sciences (SPSS) software, version 25.0.
This study was approved by the Ethics Committee at the
Universidade Católica de Pelotas under the protocol number 47807915.4.0000.5339. All participants agreed to participate in the study by providing their informed consent. For eligible participants under the age of 18, a written consent was also obtained from their parents or guardians. According to diagnostic assessments of the larger study, the participants with any psychiatric disorders were referred to a health service center. This paper complies with the STROBE reporting guideline for cross-sectional studies.
ResultsThe sample consisted of 840 pregnant women. The mean of MFA for the general sample was 98.6 (SD 11.6). Most participants belonged to middle class (N=473 [57.5%]), had 11 years or more of schooling (N=475 [56.5%]), were 30 years old or more (N=300 [35.7%]), and lived with a partner (N=670 [79.8%]). Regarding the pregnancy characteristics, N=579 (68.9%) pregnant women were in the third trimester of pregnancy, N=483 (57.5%) had previous pregnancy, and N=374 (44.5%) did not plan this pregnancy. With regards to social support, N=120 (14.3%) of the participants did not feel supported by their mothers during pregnancy and N=39 (4.6%) did not feel supported by the child's father during pregnancy. In addition, N=136 (16.2%) of the pregnant women presented tobacco abuse/dependence, N=79 (9.4%) alcohol abuse/dependence, N=127 (15.1%) had depressive symptoms, and N=279 (33.3%) had anxiety symptoms (Table 1).
Bivariate analysis showed the pregnant women who did not live with a partner (
p<0.001), were between first and second trimester of pregnancy (
p<0.001), did not plan the pregnancy (
p=0.032), did not feel supported by their mother during pregnancy (
p=0.030), did not feel supported by the child's father during pregnancy (
p=0.042), had alcohol abused/dependence (
p=0.019), had depressive symptoms (
p<0.001) and, those with anxiety symptoms (
p=0.013) presented significantly lower MFA means (Table 1).
In the adjusted analysis, was found that pregnant women who had lower MFA means were those who did not live with a partner (B=-3.9 [CI95%=-6.0; -1.7]
p<0.001), were between the first and second trimester of pregnancy (B=-4.3 [CI95%=-6.0; -2.6]
p<0.001), did not feel supported by their mother during pregnancy (B=-2.4 [CI95%=-4.6; -0.2]
p=0.035), and those women with depressive symptoms (B=-5.0 [CI95%=-7.4; -2.5]
p<0.001) (Table 2). The variables on economic class, schooling, age, previous pregnancy, previous abortion, planned pregnancy, child's father support, tobacco abuse/dependence, alcohol abuse/dependence, and anxiety symptoms were not statistically associated with MFA (
p>0.005).
DiscussionThis study explored a set of factors associated with MFA, such as social support, substance abuse, mental health, socio-demographic, and gestational characteristics in a population-based sample in the South of Brazil. It was found that pregnant women who did not live with a partner, who did not have their mother's support during pregnancy, who were between the first and second gestational trimesters, and who had depressive symptoms presented lower MFA means.
The findings have demonstrated the importance of an appropriate support network during pregnancy, especially from partners, parents, or other close family members, as reported in previous studies.
7,24,25 Puerperium is a period of great changes in women's lives. Positive social support, as well as lives with a partner during this period may contribute to improved maternal and infant well-being and can also be very helpful in facilitating bonding between mothers and their children. In terms of MFA, a mother who knows what it is like to receive support and care, may be more acceptable for care.
It was found that pregnant women who did not have their mother's support during pregnancy and who did not live with a partner had lower MFA means. However, the baby's father support variable did not remain associated with MFA in the multivariate analysis. The literature demonstrates the relevance of a partner in this important period for a woman.
4,16,26 Sometimes, the baby's father is not necessarily the mother's current partner. A study found that married women had more support than those that were unmarried, and that partner presence and marital stability are important factors for health and well-being.
26 Thus, the presence of a partner, which enables affective exchanges, a feeling of security and belonging by the pregnant woman, may be more related to the maternal ability to bond with her baby.
These results corroborate with those found in the literature. A study by Punamäki
et al.
8 involved 511 mother-child dyads and showed that social support during pregnancy and good maternal mental health have contributed to higher levels of MFA. Adequate social support during times of high stress and great vulnerability in the life cycle seems to be of great importance in several aspects. It has also been associated with protective factors for mental health.
Another important result of the present study was that pregnant women with depressive symptoms had lower MFA means. The damage of gestational depression in offspring is well established in the literature. Symptoms of depression (sadness, apathy, anhedonia, guilt, and others) can interfere with the empathic ability and the availability of maternal affection, and thus, impair to build a healthy bonding with the child.
1Rossen
et al.
9 identified the different risk and protective factors associated with maternal representations in relation to the fetus. The results showed that higher depressive symptoms were the strongest risk factors associated with the mother's negative expectations regarding to the unborn child. Another study that compared MFA in women with Major Depressive Disorder (MDD) with those without the disorder found that the diagnosis of MDD was associated with significantly lower levels of MFA. The severity of depression was negatively associated with MFA scores, indicating that the more severe the depression, the lower the MFA of the pregnant woman.
27It was also found that pregnant women who were between the first and the second trimester of pregnancy had lower MFA means. According to Cranley
5 MFA tends to intensify over the course of pregnancy due to body changes and to the increased fetal movements, which can facilitate the creation of the fetus' representations and, consequently, the bond with it. These findings corroborate with the study carried out by Rowe
et al.
28 in Australia in which pregnant women who were in the first gestational trimester had lower MFA means. In the United States, Yarcheski
7 conducted a meta-analytical study to identify predictors of maternal bonding with the fetus and to determine the magnitude of the relationship of each predictor. The study yielded fourteen predictors of MFA and gestational age had a moderate to substantial effect size, indicating that MFA intensifies with the advancing pregnancy.
The results of this study should be interpreted with some caution. The fact that it was a cross-sectional study, therefore, it was impossible to infer causality, which it could be considered a limitation of this study. In addition, although it did not find an association between MFA and alcohol and tobacco abuse, some previous studies have shown this relationship.
13,24 It is possible that, due to the pregnant women's social acceptability, many felt uncomfortable to admit the abuse of these substances, which may have interfered with our findings (interviewee bias). In addition, it should be noted that the assessment of alcohol and tobacco abuse was performed in the first phase of the study, which included women who were up to 24 gestational weeks. As the ASSIST instrument investigates the abuse of these substances in the last three months, it is possible that some women responded regarding to a period when they were not pregnant. Therefore, it was suggested further research on the subject.
Despite the limitations, a range of possible associated and confounding factors mentioned in the literature that confirm the findings of our study was investigated. Furthermore, research that explores factors that can serve as protection for the pregnancy and child development is appropriate, mainly in the most vulnerable populations. MFA has been considered an indicator of adaptation to pregnancy and associated with health practices during this period. Positive health practices include abstaining from risky behaviors such as the use of tobacco, alcohol, and other illegal substances.
13,14It is known that positive MFA contributes to the mother-child relationship after birth and especially to the development of a secure bonding towards the child.
8 Those who are securely bonded tend to be more satisfied in relationships with others.
29 Moreover, previous studies showed that MFA was directly associated with child development.
8,14 Thus, attention to MFA is justified, since there is evidence for both positive and negative influence on the offspring's outcomes .
14In this perspective, these findings support the study by Roncallo
et al.
30 who suggested that a way to early promotion in a child's development in the perinatal period includes the promotion of prenatal bonding, couple's relationship, social support networks, and the mother's physical and mental health. Thus, early evaluation of MFA is appropriate and may be a useful indicator for early clinical and psychological intervention.
12 Working to foster prenatal bond may have a positive impact on physical and emotional care patterns during that same period, as well as a better mother-infant relationship in the postpartum period.
In summary, the results of this study showed that a higher MFA was associated with an adequate support network during pregnancy, especially mother support and living with a partner. MFA was also associated with better maternal mental health and advanced pregnancy. It is noteworthy that the gestational period is characterized by several hormonal and psychosocial changes, in which pregnant women are more vulnerable emotionally. It is also during this period that the first relationship with the fetus begins. Therefore, it is essential that pregnant women feel good and safe for the development of a positive MFA. Thus, appropriate interventions in prenatal care settings should be implemented to help pregnant women to have a healthy pregnancy. These interventions should emphasize the importance of social support and maternal mental health for enabling the development and improvement of a healthy MFA.
References1. Krob AD, Godoy J, Leite KP, Mori SG. Depressão na Gestação e no Pós-Parto e a Responsividade Materna Nesse Contexto. Rev Psicol Saúde. 2017 Nov; 9 (3): 3-16.
2. DiPietro JA. Psychological and psychophysiological considerations regarding the maternal-fetal relationship. Infant Child Dev. 2010 Jan; 19 (1): 27-38.
3. Feijó MCC. Validação brasileira da "maternal-fetal attachment scale" / Brazilian validation of the maternal-fetal attachment scale. Arq Bras Psicol. 1999; 51 (4): 52-62.
4. Rusanen E, Lahikainen AR, Pölkki P, Saarenpää-Heikkilä O, Paavonen EJ. The significance of supportive and undermining elements in the maternal representations of an unborn baby. J Reprod Infant Psychol. 2018 May 27; 36 (3): 261-75.
5. Cranley MS. Development of a Tool for the Measurement of Maternal Attachment During Pregnancy. Nurs Res. 1981 Sep; 30 (5): 281-4.
6. Alvarenga P, Dazzani MVM, Alfaya CA dos S, Lordelo E da R, Piccinini CA. Relações entre a saúde mental da gestante e o apego materno-fetal. Estud Psicol (Natal). 2012 Dec; 17 (3): 477-84.
7. Yarcheski A, Mahon NE, Yarcheski TJ, Hanks MM, Cannella BL. A meta-analytic study of predictors of maternal-fetal attachment. Int J Nurs Stud. 2009 May; 46 (5): 708-15.
8. Punamäki RL, Isosävi S, Qouta SR, Kuittinen S, Diab SY. War trauma and maternal-fetal attachment predicting maternal mental health, infant development, and dyadic interaction in Palestinian families. Attach Hum Dev. 2017 Sep 3; 19 (5): 463-86.
9. Rossen L, Hutchinson D, Wilson J, Burns L, Allsop S, Elliott E,
et al. Maternal Bonding through Pregnancy and Postnatal: Findings from an Australian Longitudinal Study. Am J Perinatol. 2017 Jul 17; 34 (8): 808-17.
10. Souza GFA, Souza ASR, Praciano GAF, França ESL, Carvalho CF, Paiva Júnior SSL,
et al. Apego materno-fetal e transtornos psiquiátricos em gestantes com fetos malformados. J Bras Psiquiatr. 2022 Mar; 71 (1): 40-9.
11. Cannella BL. Maternal-fetal attachment: an integrative review. J Adv Nurs. 2005 Apr; 50 (1): 60-8.
12. Kelmanson IA. Maternal Antenatal Attachment Scale (MAAS) reference values at different stages of pregnancy and their possible associations with major obstetric and demographic characteristics. Early Child Dev Care. 2022 Jul; 192 (10): 1673-84.
13. Massey SH, Bublitz MH, Magee SR, Salisbury A, Niaura RS, Wakschlag LS,
et al. Maternal-fetal attachment differentiates patterns of prenatal smoking and exposure. Addict Behav. 2015 Jun; 45: 51-6.
14. Alhusen JL, Gross D, Hayat MJ, Nancy Woods AB, Sharps PW. The influence of maternal-fetal attachment and health practices on neonatal outcomes in low-income, urban women. Res Nurs Health. 2012 Apr; 35 (2): 112-20.
15. Santos NF, Costa RA. Parental tobacco consumption and child development. J Pediatr (Rio J). 2015 Jul; 91 (4): 366-72.
16. Rubertsson C, Pallant JF, Sydsjö G, Haines HM, Hildingsson I. Maternal depressive symptoms have a negative impact on prenatal attachment - findings from a Swedish community sample. J Reprod Infant Psychol. 2015 Mar; 33(2):153-64.
17. Foley S, Hughes C, Murray AL, Baban A, Fernando AD, Madrid B,
et al. Prenatal attachment: using measurement invariance to test the validity of comparisons across eight culturally diverse countries. Arch Womens Ment Health. 2021 Aug; 24 (4): 619-25.
18. Rosa KM, Scholl CC, Ferreira LA, Trettim JP, Cunha GK, Rubin BB,
et al. Maternal-fetal attachment and perceived parental bonds of pregnant women. Early Hum Dev. 2021 Mar; 154: 105310.
19. Santos IS, Matijasevich A, Tavares BF, Barros AJD, Botelho IP, Lapolli C,
et al. Validation of the Edinburgh Postnatal Depression Scale (EPDS) in a sample of mothers from the 2004 Pelotas Birth Cohort Study. Cad Saúde Pública. 2007 Nov; 23 (11): 2577-88.
20. Gomes-Oliveira MH, Gorenstein C, Neto FL, Andrade LH, Wang YP. Validation of the Brazilian Portuguese Version of the Beck Depression Inventory-II in a community sample. Rev Bras Psiquiatr. 2012 Dec; 34 (4): 389-94.
21. Lima Osório F, Crippa JAS, Loureiro SR. Further psychometric study of the Beck Anxiety Inventory including factorial analysis and social anxiety disorder screening. Int J Psychiatry Clin Pract. 2011 Nov; 15 (4): 255-62.
22. Henrique IFS, Micheli D, Lacerda RB, Lacerda LA, Formigoni MLOS. Validação da versão brasileira do teste de triagem do envolvimento com álcool, cigarro e outras substâncias (ASSIST). Rev Assoc Med Bras. 2004 Apr; 50 (2): 199-206.
23. Brazilian Association of Research Companies - Brazilian Economic Classification Criteria. [
Internet]. 2015. Available from: www.abep.org
24. Maas AJBM, Vreeswijk CMJM, Braeken J, Vingerhoets AJJM, van Bakel HJA. Determinants of maternal fetal attachment in women from a community-based sample. J Reprod Infant Psychol. 2014 Jan; 32 (1): 5-24.
25. Orr ST. Social Support and Pregnancy Outcome: A Review of the Literature. Clin Obstet Gynecol. 2004 Dec; 47 (4): 842-55.
26. Cohen K, Capponi S, Nyamukapa M, Baxter JK, Worly BL. Social Determinants of Partner Support in Pregnancy. Obstet Gynecol. 2014 May; 123 (Suppl. 1): 142S.
27. McFarland J, Salisbury AL, Battle CL, Hawes K, Halloran K, Lester BM. Major depressive disorder during pregnancy and emotional attachment to the fetus. Arch Womens Ment Health. 2011 Oct; 14 (5): 425-34.
28. Rowe HJ, Wynter KH, Steele A, Fisher JRW, Quinlivan JA. The Growth of Maternal-Fetal Emotional Attachment in Pregnant Adolescents: A Prospective Cohort Study. J Pediatr Adolesc Gynecol. 2013 Dec; 26 (6): 327-33.
29. Dubber S, Reck C, Müller M, Gawlik S. Postpartum bonding: the role of perinatal depression, anxiety and maternal-fetal bonding during pregnancy. Arch Womens Ment Health. 2015 Apr 5; 18 (2): 187-95.
30. Roncallo CP, Barreto FB, Miguel MS. Promotion of child development and health from the perinatal period: an approach from positive parenting. Early Child Dev Care. 2018 Nov; 188 (11): 1540-52.
Received on October 28 2022
Final version presented on January 11, 2023
Approved on February 1, 2023
Associated Editor: Sheyla Costa
Acknowledgements: We would like to express our gratitude to all the pregnant women who participated in this study. We would like to thank the Bill & Melinda Gates Foundation,
Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), and
Instituto Nacional de Ciência e Tecnologia (INCT).
Authors' contribution: Rubin BB: Conceptualization, Data Curation, Writing - Original Draft. Matos MB: Data Curation, Writing - Review & Editing. Trettim JP: Investigation, Writing - Review & Editing. Scholl CC: Data Curation, Investigation. Cunha GK: Investigation, Writing - Review & Editing. Curcio E: Validation, Investigation. Stigger RS: Investigation, Writing - Review & Editing. Martins CSR: Investigation, Data Curation. Motta JVS: Methodology, Formal analysis. Ghisleni G: Writing - Review & Editing, Project administration. Pinheiro RT: Methodology, Project administration, Funding acquisition. Quevedo LA: Writing - Review & Editing, Formal analysis, Supervision.
The authors approved the final version of the article and declare no conflict of interest.


 ; Mariana Bonati de Matos2
; Mariana Bonati de Matos2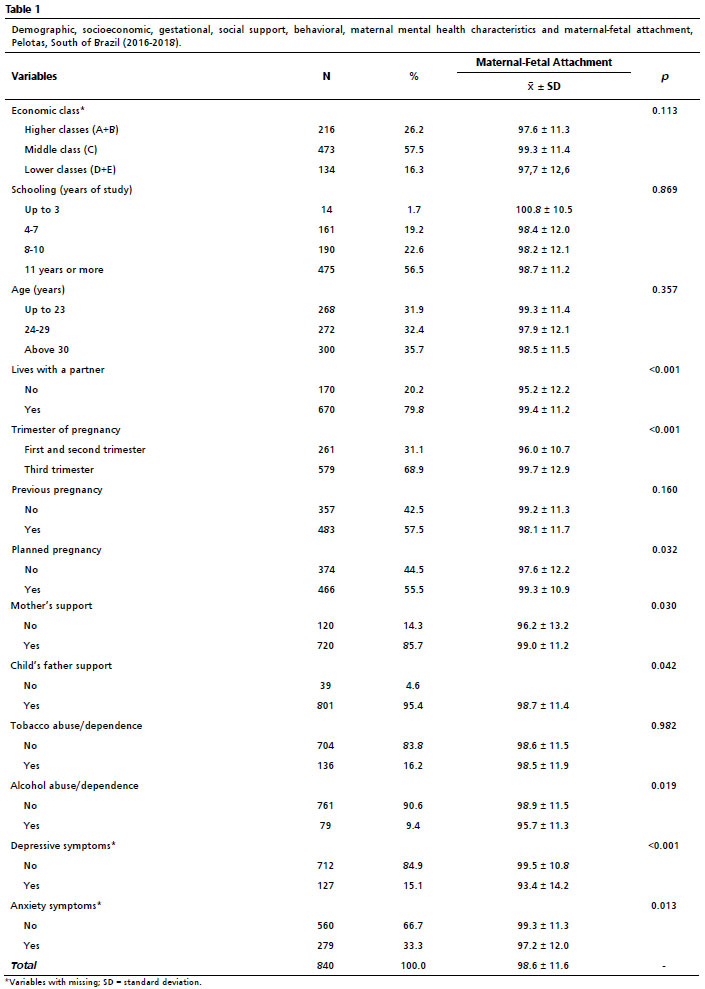






 Ler em português
Ler em português