ABSTRACT
OBJECTIVES: to analyze the factors associated with the occurrence of syphilis in pregnant women attending in Primary Health Care.
METHODS: case-control study conducted with women who underwent prenatal care in Primary Health Care. Three controls were selected for each case (48 cases and 144 controls) based on the results of serological tests for syphilis. Bivariate analysis was carried out, followed by conditional logistic regression ordered by pairs from the lowest p value.
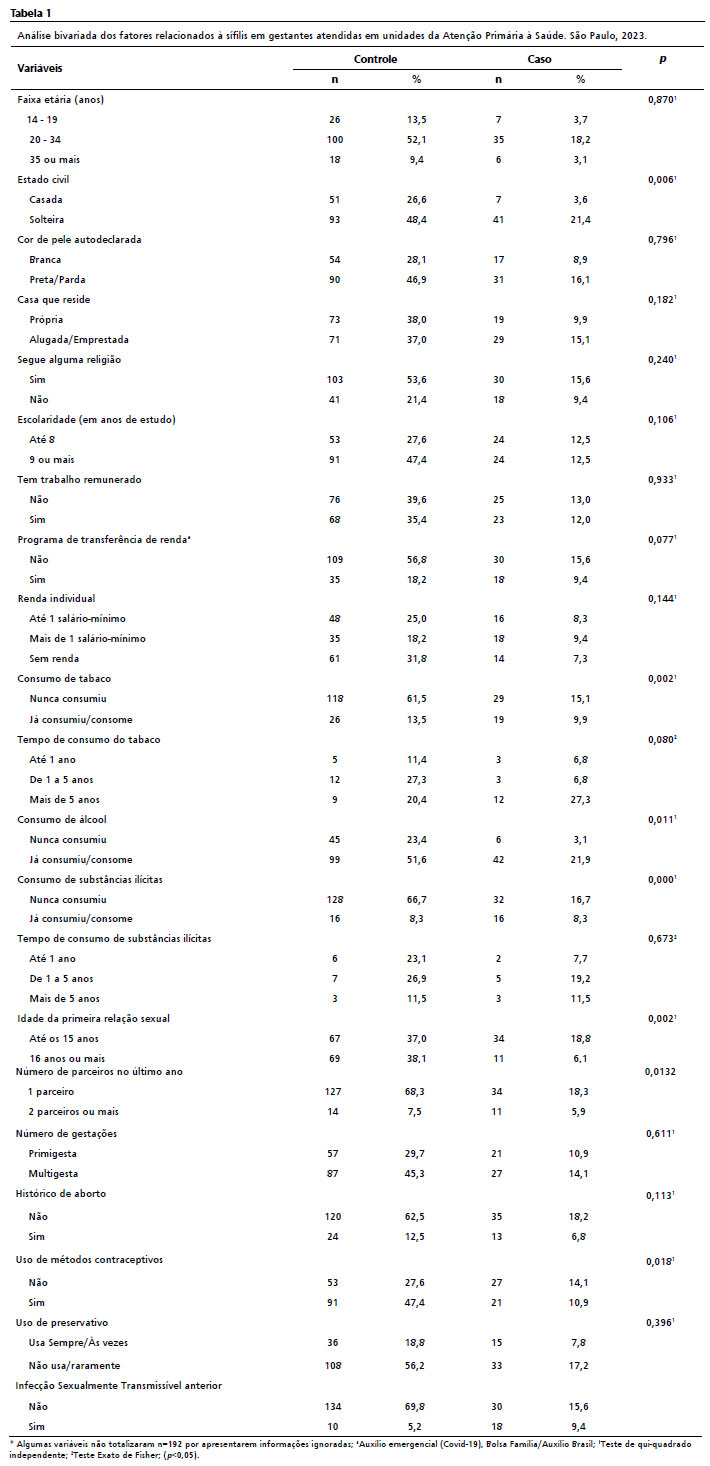
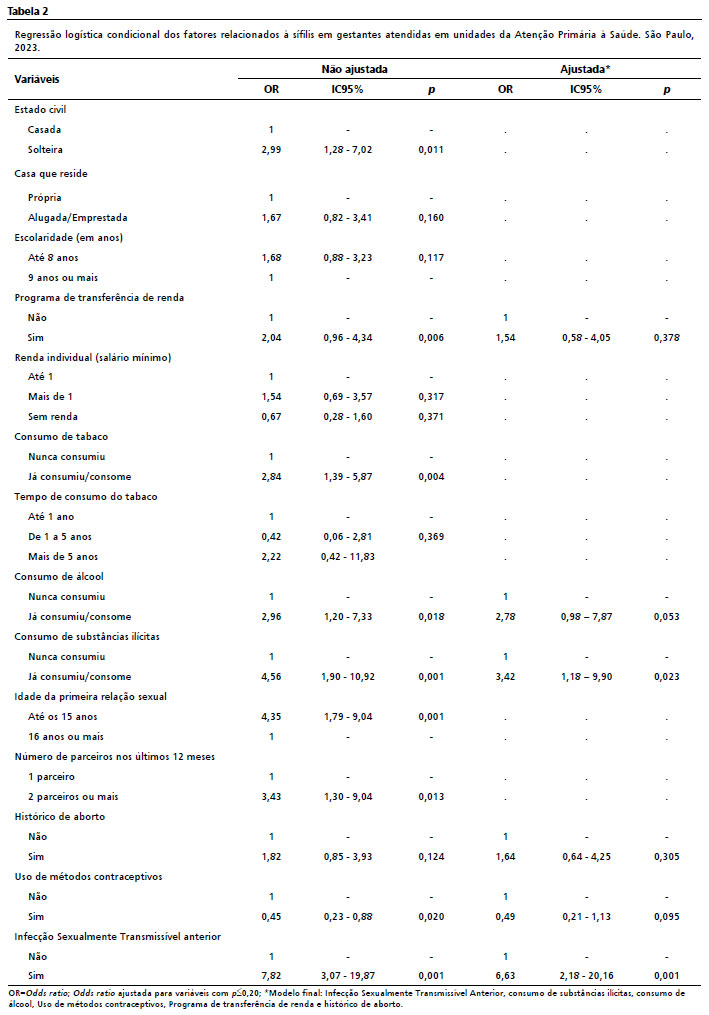
RESULTS: in the control and case groups there was a predominance of, respectively: women aged 20 to 34 (52.1%; 21.4%), single (48.4%; 21.4%), black or brown (46.9%; 16.1%), with nine or more years of schooling (47.4%; 12.5%). The associated factors were a history of illicit drug use (OR = 3.42; 95%CI= 1.18 - 9.90) and a previous diagnosis of Sexually Transmitted Infection (OR = 6.63; 95%CI=2.18 - 20.16).
CONCLUSION: the consumption of illicit substances and the presence of previous Sexually Transmitted Infection were factors associated with syphilis during pregnancy. The findings reinforce the importance of planning and reorganizing actions during prenatal care aimed at identifying and managing subjective factors, so that health services can adopt effective measures to monitor and prevent new cases of syphilis in pregnant women.
Keywords:
Sexually transmitted diseases, Pregnant women, Maternal and child health.
RESUMO
OBJETIVOS: analisar os fatores associados à ocorrência de sífilis em gestantes atendidas na Atenção Primária à Saúde.
MÉTODOS: estudo de caso-controle conduzido com mulheres que realizaram o pré-natal na Atenção Primária à Saúde. Foram selecionados três controles para cada caso (48 casos e 144 controles) a partir do resultado de testes sorológicos para sífilis. Realizou-se análise bivariada e, em seguida, regressão logística condicional ordenada por pares a partir do menor valor de p.
RESULTADOS: nos grupos controle e caso houve predomínio de, respectivamente: mulheres de 20 a 34 anos (52,1%; 21,4%), solteiras (48,4%; 21,4%), pretas ou pardas (46,9%; 16,1%), com nove ou mais anos de estudo (47,4%; 12,5%). Os fatores associados foram o histórico de consumo de substâncias ilícitas (OR = 3,42 IC95%= 1,18 – 9,90) e o diagnóstico anterior de Infecção Sexualmente Transmissível (OR = 6,63 IC95%= 2,18 – 20,16).
CONCLUSÃO: o consumo de substâncias ilícitas e a presença de Infecção Sexualmente Transmissível anterior foram fatores associados à sífilis na gestação. Os achados reforçam a importância do planejamento e reorganização de ações, durante o pré-natal, direcionadas à identificação e ao manejo de fatores subjetivos, para que os serviços de saúde possam adotar medidas eficazes no acompanhamento e prevenção de novos casos de sífilis em gestantes.
Palavras-chave:
Infecções sexualmente transmissíveis, Gestantes, Saúde materno-infantil.
IntroductionSyphilis is a Sexually Transmittable Infection (STI), which affects approximately one million pregnant women worldwide.
1,2 In Brazil, 86,111 new syphilis cases during pregnancy were notified in 2023, 46.2% of them within the state of São Paulo.
3 In spite of improvements, the infection still represents a challenge for public health due to the risk of vertical transmission and adverse outcomes (abortions, stillbirths, prematurity and congenital syphilis).
2,4Among the risk factors for gestational syphilis mentioned in the literature are social vulnerability, low educational level, lack of condom use, multiple partners, alcohol or illicit drugs use, STI history and insufficient prenatal consultations.
5-8 Such findings, stemming from studies in hospital settings, highlight the importance of surveys in primary healthcare that may explore social and behavioral aspects, and the provision of healthcare services.
Aiming at ensuring a mother and child healthcare network and mitigating mortality rates, the Ministry of Health (MH) implemented the National Policy for Humanized Childbirth and Birth, and the Stork Network (RC – Portuguese acronym for
Rede Cegonha).
9 The RC advocates for prenatal follow-up, the implementation of routine procedures with timely results, prevention of STI/HIV/Aids, the availability of rapid tests for pregnant women and their partners
4 and the decentralization of these tests to Primary Health Care (PHC). Thus, during prenatal care, all pregnant women should be screened for syphilis in the first and last trimester of pregnancy
4 and those testing positive for syphilis should be treated and followed up monthly until full recovery.
Prenatal care in PHC provides an opportunity for the promotion of a healthy pregnancy and the early identification of diseases that affect maternal-child health.
10 PHC offers a strategic environment based on patient-centered care, multidisciplinary teams, and integrated care.
9 Nevertheless, there are still challenges in the early diagnosis of syphilis during prenatal care, resulting from deficiencies in care quality, non-adherence to clinical guidelines and the lack of timely testing and adequate treatment.
6,11 Such frailties increase the risk of late diagnosis, with potential adverse outcomes.
6Considering the potential of PHC in prevention and control of gestational syphilis, studies that investigate factors associated with its occurrence at this level of care, particularly using case-control designs, are essential. In this context, the present study aimed to analyze factors associated with the occurrence of syphilis in pregnant women attended at PHC facilities.
MethodsThis is a population-based case-control study, conducted in the period from October 2020 to December 2022, with women who underwent prenatal care at PHC health facilities.
The study was conducted in two municipalities in the state of São Paulo. The first (municipality A) has a total of 71 PHC health facilities, comprising 51 Family Health Units (USF – Portuguese acronym) and 20 traditional Basic Health Units (UBS – Portuguese acronym). The second (municipality B), in turn, has a total of 36 PHC health facilities, comprising four USF and 32 UBS. We highlight that the difference in the percentage of participants between the two municipalities was a consequence of easier access to health facilities in municipality A compared to municipality B.
For sample calculation, we used the statistical freeware EPI Info version 7.2.5.0, and this estimation was performed based on a case-control study conducted in Recife,
6 considering significance level, statistical power, case-control proportion and proportion of exposed controls. Thus, we adopted a 5% significance level, an 80% statistical power, an estimated Odds Ratio (OR) of 4.16 and a 7.1% proportion of controls, considering behavioral aspects, such as drug use. We selected three controls for each syphilis case during pregnancy (3:1) and the estimated final sample was 168 women (42 cases and 126 controls). Expecting the possibility of a 20% sample loss, we estimated that 200 participants would be necessary, comprising 50 cases and 150 controls.
We selected women aged 12 to 49 years (childbearing age), who resided in any of the municipalities of the study, were at any stage of the pregnancy period and were receiving prenatal care at PHC facilities. We also included women who had babies up to six months of age receiving follow-up through well-child care in these facilities. We excluded those who were at the facility for their first prenatal care consultation, had not yet received serological tests results, or were not receiving prenatal care in PHC services.
The case group consisted of women who had a reactive result, regardless of the titer, in serological tests for syphilis. (
Fluorescent Treponemal Antibody Absorption - FTA-ABS – or
Venereal Disease Research Laboratory - VDRL), performed during prenatal care of the current period of pregnancy. The control group consisted of women who had non-reactive results from syphilis serological tests (FTA-ABS or VDRL), performed during prenatal care, and who had no syphilis diagnosis during the current pregnancy. The selection of participants from the control group was performed randomly, in the same health facility, after the identification of the case.
The group matching was performed based on the type of facility (USF/UBS), the municipality (A or B) and the statuses of participants (pregnant women or women with infants up to six months of age at the time of data collection). The inclusion of seropositive women who were currently pregnant or had already given birth occurred due the interruption of data collection during the COVID-19 pandemic. Matching between case and control groups was also performed based on the infant's age.
For data collection, we initially performed a survey at the municipal epidemiological surveillance of health facilities with cases of syphilis in pregnant women, without access to the name of notified cases. The facilities with positive cases were included in the study and periodically contacted by researchers for the physical approach of the potential participants.
Pregnant women and/or those who had infants of up to six months of age present in the health facility on the day of the visit – for consultation, vaccination, pregnant women group – were individually approached. The approach was conducted exclusively in health facilities, according to the methodology of a previous study,
12 aiming to maintain diagnostic privacy and avoid discomfort associated with home visits.
The interviews were carried out based on a structured questionnaire, which encompasses socioeconomic, demographic, health-behavioral and obstetric data, and information on syphilis diagnosis in the current pregnancy. We approached 209 women, and the final sample size was composed of 192 participants (Figure 1).
The outcome of the study was the presence of syphilis during the current pregnancy. The dependent variables were grouped into three clusters: (i) demographic and socioeconomic (age, marital status, self-declared skin color, schooling, type of residence, paid work, enrollment in income transfer programs, and individual income and religion); (ii) health behaviors (consumption of tobacco, alcohol and illicit drugs, age of the first sexual intercourse, number of sexual partners in the previous year, use of contraceptive methods and condom) and; (iii) obstetric (number of pregnancies, abortion history and presence of previous STI).
Data obtained were analyzed with Stata 14.0 software. We performed a descriptive analysis using frequency, mean and standard deviation, followed by bivariate analyses (Chi-square test and Fisher's Exact Test). Variables with
p<0.20 were included in the conditional logistic regression model, ordered in pairs from the lowest
p value. The variables abortion and contraceptive methods were maintained in the model due to adjustment factors. Collinearities between variables were tested.
For validation, we used non-conditional logistic regression, including variables similarly to the conditional logistic regression. The associations were expressed by Odds ratio (OR), with a 95% confidence interval and a 5% level of significance.
The study was approved by the Research and Ethics Committee (CAAE protocol: 28783320.3.0000.5418).
ResultsThis study included 192 pregnant women and/or women with infants up to six months of age, recruited from 16 PHC facilities. Of these, 87.5% (n=168) were from municipality A and 12.5% (n=24) from municipality B.
In both groups, the majority of women were aged 20 to 34 years, were single, self-declared Black or Brown, and had nine or more years of schooling. With regard to individual income, the majority of women did not have any income in the control group and had more than one minimum wage in the case group. Concerning factors associated with syphilis diagnosis in the current pregnancy, it was associated with marital status; use of tobacco, alcohol or illicit drugs; age of the first sexual intercourse; use of contraceptive methods, and presence of previous STI (Table 1).
Among the interviewees, we observed that the majority reported not using condoms during sexual intercourse, in both case and control groups. Among the main reasons described by the participants were: the woman or her partner does not enjoy using condom while having sexual intercourse, being in stable union or having a regular partner and use of contraceptive methods.
In the logistic regression analysis, the non-conditional model used demonstrated results consistent with those observed in the conditional model and they were, thus, compatible with the hypothesis of model validity. In this way, the adjusted model demonstrated that the odds ratio for syphilis in pregnancy was 3.42 times higher among participants who used illicit drugs (95%CI=1.18 – 9.90) and 6.63 times for pregnant women who already were diagnosed previously with any STI (95%CI= 2.18 – 20.16) (Table 2).
DiscussionThe findings of this research indicate that, among the participants who had prenatal care in the investigated facilities, the occurrence of syphilis in pregnancy was associated with previous STI and illicit drug history.
Schooling and income are determinants of an adequate prenatal care, influencing the access to services and the comprehension of healthcare guidelines.
7,23 However, we observe an increasing syphilis incidence among women with higher schooling.
14 Thus, it is essential that socioeconomic and demographic aspects are considered at prenatal consultations, aiming to promote inclusion, access to comprehensible information and the active participation pregnant women, their partners and their support networks in the prevention, diagnosis and treatment of STIs such as syphilis.
Although these variables are understood as associated with syphilis during pregnancy,
6,8-15, this study did not find such a relationship, possibly due to the increase of schooling, higher access to the Unified Health System (SUS – Portuguese acronym) or the sample homogeneity. In this context, an approach that goes further the traditional protocol is necessary, such as tests and number of consultations. Prenatal care should be a moment of sharing and building of knowledge, and, accordingly, investing in educational activities, particularly by means of the knowledge translation,
17 is a priority strategy.
With regard to the health behavior variables, it was evidenced that they were associated with the occurrence of syphilis in pregnant women, however, in the final model, only illicit drug use and presence of previous STI were statistically significant. These findings, aligned with other studies,
6,8,18 reinforce the importance of considering these variables as potential predictors and a point of attention in prenatal care.
Regarding alcohol use, it may increase the risk/odds of syphilis seropositivity threefold.
19,20 In the present study, there was an association only in the bivariate analysis, which lost significance in the adjusted model, in consonance with a previous study.
6 Notwithstanding, its indirect effects are still relevant, given its concomitant use with illicit drugs and its negative impact in risk perception and decision making, which may favor the exposition to infection.
21The use of illicit drugs was associated with syphilis, in alignment with studies conducted in Brazil
6 and United States,
18 which indicated a higher risk for pregnant women who started the use before 18 years old and the risk factor for congenital syphilis occurrence. The transmission of STIs in this context may occur directly, by means of sharing needles and syringes, or indirectly, through risky sexual behaviors,
22 such as the non-use of condom and having multiple partners.
The absence of knowledge on effects of illicit drugs use on their own health and the health of children may lead pregnant women to not adhere prenatal care.
21,23 Furthermore, factors such as the easy access to these drugs, vulnerable family context, fear of stigmatization and lack of preparedness of health professionals impair the early identification of the use and risky practices, compromising the harm prevention to the mother-baby dyad.
23,24Previous STIs history was significantly associated with syphilis during pregnancy, reinforcing findings of other Brazilian studies
6,25 and highlighting the risk of reinfection. Given the above, the prenatal follow-up should consider this history, particularly in low-titer syphilis cases, to identify relapses, to prevent new cases, and thus, reducing congenital syphilis cases.
25 Furthermore, educational PHC actions are essential to promote autonomy, dialog and effective strategies of prevention among pregnant women and their partners.
26 The participation of the partner in prenatal consultations is essential to the diagnosis and treatment of infections such as syphilis, preventing reinfections. Since 2016, the MH instituted the prenatal care of the partner, in attempt to promote regular tests, rapid tests, vaccination and recommendations about the role of the partner in this period.
10,27 Therefore, it is primordial that the participation of the partner is encouraged,
26 since the performance of routine tests favors diagnosis and treatment of infections, when they are present. However, regarding STIs seropositivity, the literature is still limited concerning the manner that the communication of the diagnosis to the partner occurs, and its effectiveness, which may negatively affect the adherence and treatment.
28In this context, we highlight the role of PHC in combating syphilis, particularly in prenatal care. From 2012 to 2018, the federal government expanded the coverage and encouraged the qualification of services, in order to improve diagnosis, management and treatment of the infection.
27,29 A research about syphilis management in PHC evidenced improvements in infrastructure and work processes, in addition to revealing regional inequalities and scarcity of structured teams.
29 The insufficiency of human resources, rapid tests and penicillin compromises the effectivity of integrated care, including the adherence of partners to the treatment. The PHC qualification is essential with regard to the building of bonds between pregnant women and their partners, favoring the identification of risks, screening, diagnosis, prevention and continuity of care, which are essential elements for syphilis control at SUS.
27As a limitation, we highlight the social desirability information bias, mostly with regard to sexual behavior, due to the trend of socially acceptable answers in sensitive subjects.
29,30 In order to mitigate this bias, the interviews were performed by a single researcher, in a confidential environment that assured privacy; another limitation was the restriction of the sample to users of PHC facilities, which decreases data generalization. This limitation was minimized by the case-control design and the sample matching concerning income and schooling. We also highlight that, since it is a retrospective study, we did not consider the possibility of syphilis seroconversion in the control group until the end of pregnancy, recommending further prospective studies in order to deepen the comprehension about the infection.
Even considering the potential limitations, we highlight the importance of this study for the identification of factors associated with the diagnosis of syphilis in pregnancy, as well as the possibility of interventions even at the PHC level, with the aim of promoting infection control among this group, also preventing new cases.
The results indicated that the use of illicit drugs and previous STI history were the main factors associated with syphilis in pregnancy among women receiving care at PHC. Given the central role of PHC as the entry point to the health system, the study highlights importance of quality care and the early identification of these factors by professionals, to facilitate timely interventions and the prevention of adverse outcomes resulting from seropositivity.
This study also reinforces the need for educational initiatives and the strengthening of pregnant women's autonomy, in addition further studies examining integrated care, from diagnosis to cure.
References1. World Health Organization (WHO). WHO guideline on Syphilis screening and treatment for pregnant women. Geneva: WHO; 2017. [access in 2023 Fev 20]. Available from:
http://apps.who.int/iris/bitstream/10665/259003/1/9789241550093-eng.pdf?ua=12. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Boletim Epidemiológico: Sífilis 2024. Brasília (DF): Ministério da Saúde; 2024. [access in 2025 Jun 2]. Available from:
https://www.gov.br/aids/pt-br/central-de-conteudo/boletins-epidemiologicos/2024/boletim_sifilis_2024_e.pdf/view3. Ministério da Saúde (BR). Portaria nº 1459, de 24 de Junho de 2011. Institui, no âmbito do Sistema Único de Saúde - SUS - a Rede Cegonha. DOU, Brasília, 27 jun. 2011. Seção 1. [access in 2023 Fev 20]. Available from:
http://bvsms.saude.gov.br/bvs/saudelegis/gm/2011/prt1459_24_06_2011.html4. Rosa LGF, Santos FS, Vatam CM, Burg MR, Camargo MIB. Análise do rastreamento oportuno da sífilis no pré-natal de baixo risco. Aletheia. 2020, 53 (1): 133-45.
5. Pitilin EB, Gasparini VA, Silva DTR, Souza JB. Haag FB. Hospitalizations due to Congenital Syphilis in Neonates: Associated Factors from the Prenatal Care Process. Aquichan. 2020; 20 (40): e2048.
6. Macêdo VC, Lira PIC, Frias PG, Romaguera LMD, Caires SFF, Ximenes RAA. Fatores de risco para sífilis em mulheres: estudo caso-controle. Rev Saúde Pública. 2017, 51: 78.
7. Cesar JA, Camerini AV, Paulitsc RG, Terlan RJ. Não realização de teste sorológico para sífilis durante o pré-natal: prevalência e fatores associados. Rev Bras Epidemiol. 2020, 23: e200012.
8. Moura JRA, Bezerra RA, Oriá MOB, Vieira NFC, Fialho AVM, Pinheiro AKB. Epidemiology of gestational syphilis in a Brazilian state: analysis in the light of the social-ecological theory. Rev Esc Enferm USP. 2021; 55: e20200271.
9. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Doenças de Condições Crônicas e Sexualmente Transmissíveis. Manual técnico para o diagnóstico da sífilis. Brasília (DF): Ministério da Saúde; 2021. [access in 2023 Jun 20]. Available from:
https://www.gov.br/aids/pt-br/centrais-de-conteudo/publicacoes/2021/manual-tecnico-para-o-diagnostico-da-sifilis10. Marques BL, Tomasi YT, Saraiva SS, Boing AF, Geremia DS. Orientações às gestantes no pré-natal: a importância do cuidado compartilhado na atenção primária em saúde. Esc Anna Nery. 2021; 25 (1): e20200098.
11. Lima VC, Mororó RM, Martins MA, Ribeiro SM, Linhares MSC. Perfil epidemiológico dos casos de sífilis congênita em um município de médio porte do nordeste brasileiro. J Health Biol Sci. 2017; 5 (1): 56-61.
12. Vicente JB, Sanguino GZ, Riccioppo MRPL, Santos MRD, Furtado MCC. Syphilis in pregnancy and congenital syphilis: women's experiences from the perspective of symbolic interactionism. Rev Bras Enferm. 2022 Nov; 76 (1): e20220210.
13. Araújo MAL, Andrade RFV, Barros VL, Bertoncini MRP. Fatores associados aos desfechos desfavoráveis provocados pela Sífilis na gestação. Rev Bras Saúde Matern Infant. 2019, 19 (2): 421-9.
14. Correia DM, Soares MF, Júnior JNO, Machado MF. Sífilis materna e congênita: ainda um desafio. Cad Saúde Pública. 2013, 8 (3): 221-38.
15. Magalhães DMS, Kawaguchi IAL, Dias A, Calderon IMP. Sífilis materna e congênita: ainda um desafio. Cad Saúde Pública. 2013; 29 (6): 1109-20.
16. Viacava F, Oliveira RAD, Carvalho CC, Laguardia J, Bellido JG. SUS: supply, access to and use of health services over the last 30 years. Ciên Saúde Colet. 2018 Jun; 23 (6): 1751-62.
17. Pina-Oliveira AA, Moreira RL, Pécora RAF, Chiesa AM. Análise do processo de translação do conhecimento sobre a primeira infância no ensino de graduação. Rev Esc Enferm USP. 2014; 48 (Esp): 164-71.
18. Ghanem KG, Ram S, Rice PA. The Modern Epidemic of Syphilis. N Engl J Med. 2020 Feb 27; 382 (9): 845-54.
19. Neta ME, Silva CSDO, Silva Junior RFD, Eleutério TP, Holzmann APF, Ruas EDFG, Marques LO. Prevalência e fatores associados à sífilis em gestantes atendidas na atenção primária à saúde de um município do sudeste do Brasil. Rev Bras Saúde Matern Infant. 2024; 24, e20230188.
20. Enbiale M, Getie A, Haile F, Tekabe B, Misekir D. Magnitude of syphilis sero-status and associated factors among pregnant women attending antenatal care in Jinka town public health facilities, Southern Ethiopia, 2020. PLoS One. 2021; 16 (9): e0257290.
21. Neta ME, Silva CSO, Silva Junior RF, Eleutério TP, Holzmann APF, Ruas EFG, et al. Prevalência e fatores associados à sífilis em gestantes atendidas na atenção primária à saúde de um município do sudeste do Brasil. Rev Bras Saúde Mater Infant. 2024; 24: e20230188.
22. Lin KW. Closing Primary and Prenatal Care Gaps to Prevent Congenital Syphilis. Am Fam Physician. 2020 Jul; 102 (2): 78-9.
23. Portela GLC, Barros LM, Frota NM, Landim APP, Caetano JÁ, Farias FLR. Percepción de la embarazada sobre el consumo de drogas ilícitas en la gestación. Rev Eletrônica Saúde Mental Álcool Drogas. 2013; 9 (2): 58-63.
24. Oliveira EM, Souza AG, Silva EM, Costa JBC, Aguiar CC, Rodrigues CS, et al. Implantação, desenvolvimento e desafios do observatório de saúde mental e política sobre drogas: relato de experiência. Cid em Ação Rev Ext Cult. 2022 6 (2).
25. Rigo FL, Romanelli RMC, Oliveira IP, Anchieta LM. Assistência e fatores educacionais associados a sífilis congênita em uma maternidade referência: um estudo caso-controle. Rev Bras Saúde Matern Infant. 2021; 21 (1): 139-49.
26. Paiva CCN, Cardoso R. Avaliação de implantação das ações de saúde sexual e reprodutiva na Atenção Primária: revisão de escopo. Esc Anna Nery. 2020; 24 (1): e20190142.
27. Ramos Jr AN. Persistência da sífilis como desafio para a saúde pública no Brasil: o caminho é fortalecer o SUS, em defesa da democracia e da vida [Editorial]. Cad Saúde Pública. 2022; 38 (5): PT069022.
28. Figueiredo DCMM, Figueiredo AM, Souza TKB, Tavares G, Vianna RPT. Relação entre oferta de diagnóstico e tratamento da sífilis na atenção básica sobre a incidência de sífilis gestacional e congênita. Cad Saúde Pública. 2020; 36 (3): e00074519.
29. Saes MO, Duro SMS, Gonçalves CS, Tomasi E, Facchini LA. Assessment of the appropriate management of syphilis patients in primary health care in different regions of Brazil from 2012 to 2018. Cad Saúde Pública. 2022, 38(5): EN231921.
30. Bispo Junior JP. Viés de desejabilidade social na pesquisa qualitativa em saúde. Rev Saúde Pública. 2022, 56: 101.
Authors' contribution: Lino CM: manuscript design, data analysis and interpretation, writing of the manuscript. Maeda ST and Batista MJ: planning, orientation and design of the manuscript, data analysis and interpretation, manuscript review. Antunes JLF and Souza MLR: data interpretation, manuscript review. All authors approved the final version of the article and declared no conflicts of interest.
Data availability: All data supporting the results of this study were published in the article itself.
Received on September 7, 2023
Final version presented on June 5, 2025
Approved on July 2, 2025
Associated Editor: Aurélio Costa


 ; Sayuri Tanaka Maeda2
; Sayuri Tanaka Maeda2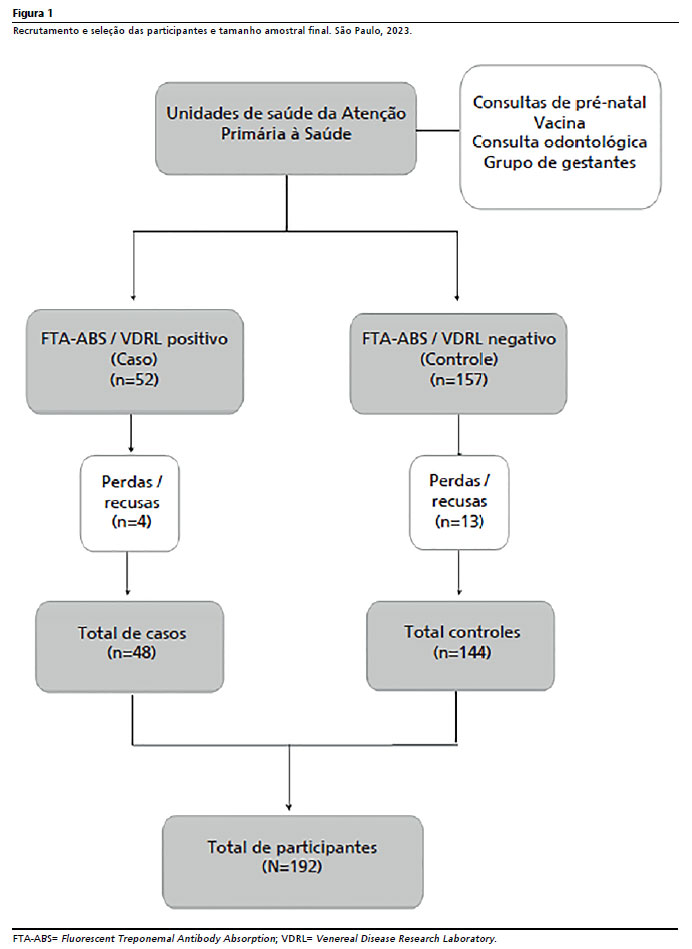






 Ler em português
Ler em português