ABSTRACT
OBJECTIVES: to identify factors associated with long hospital stays among preterm newborns.
METHODS: this is a retrospective cohort study, conducted in an outpatient clinic monitoring high-risk newborns in Northern Minas Gerais. All morbidities in the group were recorded according to the prematurity classification. Long stay was defined based on the last quartile of times, in days of stay, for the group evaluated. The variables associated with long hospital stay were defined using bivariate analysis followed by binary logistic regression, with only variables with a significance level of 5% remaining in the final model.
RESULTS: 293 newborns participated in this study, 56.6% of whom were male. The gestational age of the group ranged from 24 to 36 weeks, and 25.3% were extremely preterm. The main morbidities were related to respiratory and infectious disorders. Long stays were recorded for 25.9% of preterm newborns and the associated factors were gestational age (p<0.001), birth weight (p<0.001), late-onset sepsis (p<0.001) and necrotizing enterocolitis (p=0.036).
CONCLUSION: the factors associated with long stays highlight the need for greater vigilance in prenatal care, with safe monitoring of pregnancy and prevention of prematurity, and post-natal care, with strict surveillance in the prevention of nosocomial infections.
Keywords:
Infant premature, Morbidity, Length of stay, Neonatal intensive care units
RESUMO
OBJETIVOS: identificar fatores associados à longa permanência hospitalar entre recém-nascidos prematuros.
MÉTODOS: trata-se de estudo de coorte retrospectivo, conduzido em ambulatório de seguimento de recém-nascidos de alto risco do norte de Minas Gerais. Todas as morbidades do grupo foram registradas segundo a classificação de prematuridade. Longa permanência foi definida a partir do último quartil dos tempos, em dias de permanência, para o grupo avaliado. As variáveis associadas à longa permanência foram definidas por análises bivariadas seguidas de regressão logística binária, permanecendo no modelo final apenas as variáveis com nível de significância de 5%.
RESULTADOS: participaram deste estudo 293 recém-nascidos, sendo 56,6% do sexo masculino. A idade gestacional variou de 24 a 36 semanas, sendo 25,3% prematuros extremos. As principais morbidades foram referentes a distúrbios respiratórios e infecciosos. A longa permanência foi registrada para 25,9% dos prematuros e os fatores associados foram idade gestacional (p<0,001), peso ao nascimento (p<0,001), sepse tardia (p<0,001) e enterocolite necrosante (p=0,036).
CONCLUSÃO: os fatores associados à longa permanência destacam a necessidade de maior vigilância aos cuidados pré-natais, com acompanhamento seguro da gestação e prevenção da prematuridade, e pós neonatais, com maior cuidado à prevenção de infecções nosocomiais.
Palavras-chave:
Recém-nascido prematuro, Morbidade, Tempo de internação, Unidades de terapia intensiva neonatal
IntroductionPrematurity is the leading cause of infant mortality in various parts of the world, including Brazil, and therefore requires constant surveillance. The risk of mortality for preterm newborns (NB) varies according to several factors, including the classification.
1 Based on gestational age, the NB can be classified as extreme preterm (less than 28 weeks), very preterm (28 to 31 weeks) and moderate to late preterm (32 to 36 weeks).
2,3The first weeks of life for preterm NBs, particularly those with very low birth weight and/or who are more premature, are characterized by a heightened risk of complications due to the significant fragility of this group. They require specialized care during this critical stage, as it can have lifelong implications.
3 The most prevalent complications and intercurrent conditions for low-birth-weight newborns include respiratory, cardiac, neurological, and infectious issues.
1-4 In this context, Neonatal Intensive Care Units (NICUs) have played an increasingly significant role in reducing infant morbimortality, and their absence may lead to harmful implications.
5 In NICUs, the aim is to provide appropriate surveillance, treatment, and care for high-risk newborns, especially preterm infants who present with special care needs or require highly complex treatments.
The limit of viability has been observed for newborn situations with increasingly lower gestational ages. This translates to higher risks for this group and a prolonged hospital stay in the NICU.
1-3 It is not uncommon for complications or morbidities arising in NICUs to result in sequelae or necessitate follow-up after hospital discharge.
5-7 Specialized outpatient clinics, staffed by multidisciplinary teams, provided ongoing follow-up for NBs after NICU discharge. The results observed from these high-risk NB follow-up outpatient clinics can provide appropriate and timely feedback to both the professionals and services within the NICUs. However, there is a scarcity of studies on this topic within the national literature.
8The length of hospital stay in NICUs is a relevant aspect in the care provided after discharge and a poorly studied variable.
5,9,10 A prolonged hospitalization in NICUs leads to several impacts. These include the direct consequences of a neonate's exposure to a noisy environment, with intense light and the risk of acquiring infections,
11 as well as interferences in parental relationships, such as long family distancing, compromised breastfeeding and increased hospital costs.
12Some actors argue that fundamental aspects of preterm infant care can influence the length of hospital stay beyond what would be expected in cases of prematurity.
5,9,10,13 This study aimed to characterize the hospital morbidity profile and identify factors associated with prolonged NICU stay for preterm infants receiving care in a high-risk outpatient clinic in northern Minas Gerais.
MethodsThis is a retrospective cohort study conducted at a high-risk newborn outpatient clinic that serves infants discharged from NICUs in Montes Claros, a hub city in northern Minas Gerais. The region, with a territorial extension larger than several Brazilian states and encompassing over 80 municipalities, has a sole outpatient clinic for the follow-up of high-risk newborns, who occasionally experience prolonged stays in NICUs. Children are sent to the outpatient clinic after NICU discharge through a referral process that details birth conditions and hospital stay history, and are then followed-up by a multidisciplinary team.
The study population was composed of preterm newborns followed-up in the outpatient clinic from March 2014 to July 2018, regardless of their birthweight. Inclusion criteria were: a recorded gestational age of less than 37 weeks. Children with severe malformations or residing in other cities were excluded. For the sample calculation, following statistical models,
14 we considered a 95% confidence level, an 80% statistical power, a 1:3 ratio of exposed to unexposed and risk ratio of two, which defined a minimum number of 290 neonates for follow-up.
Data collection was conducted by medical students, supervised by a neonatologist and the data collection form, a structured, paper-based one, which was specially developed for this study, containing information on pregnancy and birth conditions (maternal hypertension, diabetes and urinary tract infections, prenatal corticosteroid, use gestational age, newborn sex, birthweight according to the classification that establishes extreme low weight as below 1000 grams, very low weight between 1000 and 1499 grams and low weight from 1500 to 2499 grams
15 and delivery room resuscitation), complications/morbidities observed during NICU stay (apneas, bronchopulmonary dysplasia, early and late-onset sepsis, intracranial hemorrhage (ICH), necrotizing enterocolitis (NEC) and hemodynamic instability).
Apneas were defined as respiratory pauses affecting in heart rate or oxygen saturation, as recorded by the healthcare team.
16 Bronchopulmonary dysplasia was defined for neonates as the need for supplemental oxygen therapy for a period equal to or greater than 28 days or 36 weeks of corrected gestational age.
17 Early-onset sepsis was defined based on diagnosis recorded in the chart for a compatible clinical picture with an onset occurred in the first 72 hours of life; and late-onset sepsis for a diagnosis recorded after 72 hours of life.
18 Sepsis was defined based on the medical diagnosis and the treatment used, regardless of the results of blood cultures. Intracranial hemorrhages were recorded based on the diagnosis and imaging findings. Necrotizing enterocolitis was assessed based on the records in charts, and hemodynamic instability was considered for cases requiring vasoactive amines.
The response variable was long stay. This is a poorly explored variable in the literature, and lacks a standardized definition. For the purpose of this study, the length of stay in the NICU for all evaluated newborns was distributed into quartiles, with a long stay being defined as the length of stay within the last quartile.
9,10After data collection, the IBM-SPSS for Windows version 22.0 software was used for data entry, processing and analysis. Frequency distributions of the main variables and morbidities were performed according to gestational age. Distribution analysis was conducted using Pearson's chi-square test, assuming a 5% significance level (
p<0.05). The variables associated with long stay were defined using bivariate analysis, followed by binary logistic regression analysis. For the multiple analysis, variables with an association up to a 20% significance level (
p<0.20) in the bivariate analyses were considered. In the final model, only variables with a 5% significance level (
p<0.05) were maintained, with their respective odds ratios and 95% confidence intervals recorded.
The research project, which forms the basis of the information presented here, was approved by the Research Ethics Committee of the State University of Montes Claros (Unimontes – Portuguese acronym), under opinion number 1.800.915.
ResultsA total of 293 newborns participated in the study. The majority of the group was male (n=163, 55.5%), and were moderate or late preterm, with a gestational age of 32 to 36 weeks (n=148; 50.5%). Regarding pregnancy and birth conditions, prenatal corticosteroids were used in 134 mothers (45.7%), the most frequent type of delivery was cesarean section (64.3%) and 56 neonates (19.1%) required resuscitation at birth.
The most frequent morbidities and complications during stays in NICUs were: Respiratory Distress Syndrome – RDS (93.9%), early-onset sepsis (48.1%), apnea (39.2%), late-onset sepsis (21.5%), bronchopulmonary dysplasia (21.2%) and hemodynamic instability (20.5%). The distribution of the main clinical conditions and complications are exposed in Table 1, according to gestational age, which also records the most common conditions or complications that were statistically associated with gestational age.
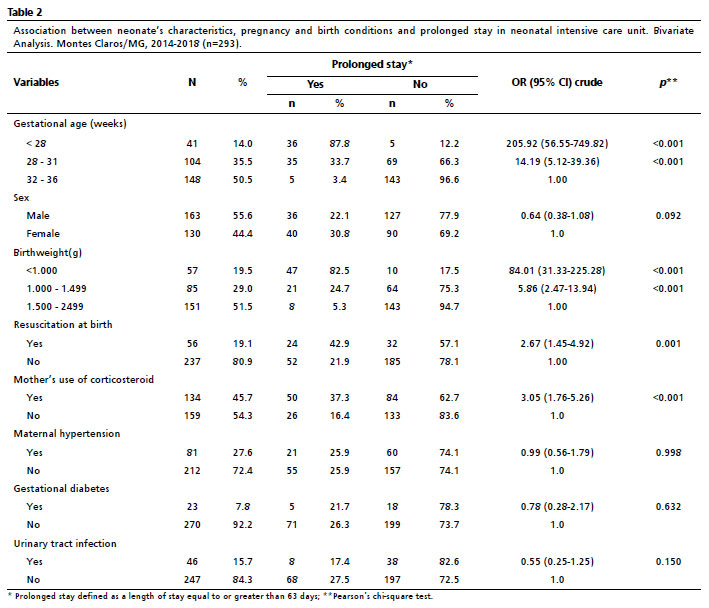
The stay in the NICUs varied from three to 347 days for the assessed group, with a median of 37 days. Of the NB's total, 76 (25.9%) had a period of stay equal to or greater than 63 days (final quartile for the total of days hospitalized), which defines long NICU stay. Table 2 shows the results of bivariate analyses between newborns' characteristics and pregnancy and birth conditions and long stay.
In this stage, variables that were statistically associated were: gestational age <28 weeks (OR=205.92; 95%CI = 56.55-749,82;
p<0.001); gestational age of 28 to 31 weeks (OR = 14.19; 95%CI =5.12-39.36;
p<0.001); birthweight <1000g (OR=84.01; 95%CI=31.33-225.28;
p<0.001); birthweight of 1000 to 1499g (OR=5.86; 95%CI = 2.47-13.94;
p<0.001); resuscitation at birth (OR=2.67; 95%CI=1.45-4.92;
p=0.001) and mother's use of corticosteroid (OR=3.05; 95%CI=1.76-5.26;
p<0.001).
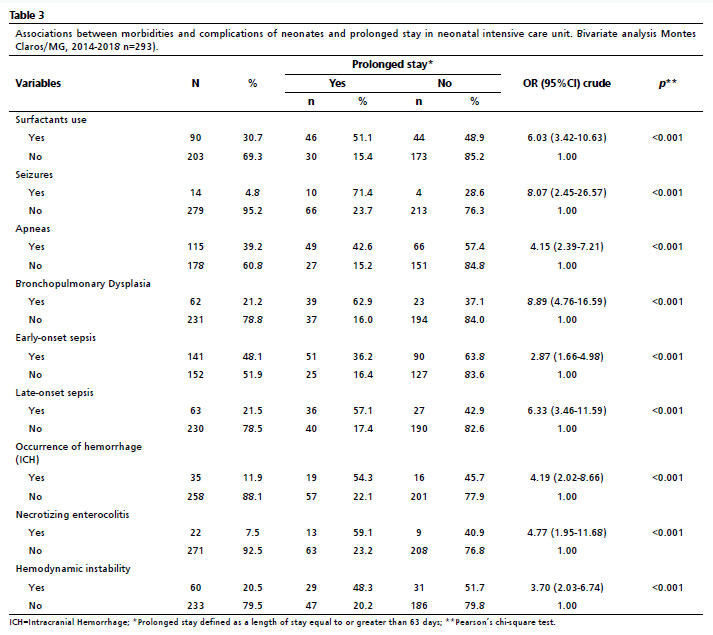
Table 3 shows the association of the most frequent morbidities and complications among the newborns observed, with long stay. On this stage of bivariate analyses, all morbidities and complications were associated with long stay = Use of surfactants (OR=6.03; 95%CI = 3.42-10.63;
p<0.001); Seizures (OR=8.07; 95%CI = 2.45-26.57;
p<0.001); Apneas (OR=4.15; 95%CI= 2.39-7.21;
p<0.001); Bronchopulmonary Dysplasia (OR=8.89; 95%CI = 4.75-16.59;
p<0.001); Early-onset sepsis (OR=2.87; 95%CI = 1.55-4.98;
p<0.001); Late-onset sepsis (OR=6.33; 95%CI = 3.46-11.59;
p<0.001) ICH (OR=4.19; 95%CI = 2.02-8.66;
p<0.001); NE (OR=4.77; 95%CI = 1.95-11.68;
p<0.001) and Hemodynamic Instability (OR=3.70; 95%CI = 2.03-6.74;
p<0.001)
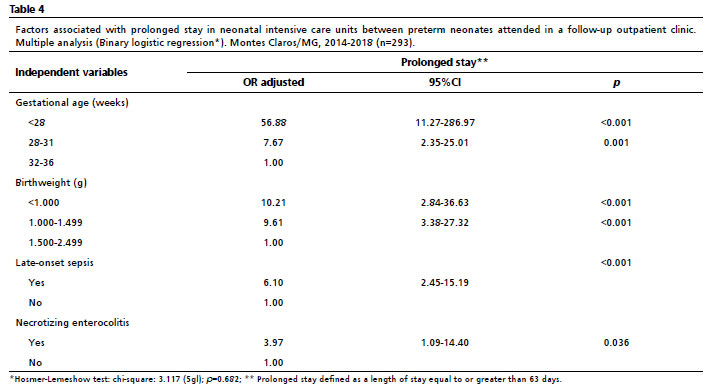
After multiple analysis, the variables gestational age, including that of under 28 weeks (OR=56.88; 95%CI = 11.27-286-97;
p<0.001), as well as that of 28 to 31 weeks (OR=7.67; 95%CI = 2.35-25.021;
p=0.001); the birthweight, including that under 1000g (OR=10.21; 95%CI= 2.84-36.63;
p<0.001) as well as that of 1000 to 1499g (OR=9.61; 95%CI = 3.38-27.32;
p<0.001); early-onset sepsis ((OR=6.10; 95%CI =2.45-15.19;
p<0.001) and necrotizing enterocolitis (OR=3.97; 95%CI =1.09 -14.04;
p=0.036) had statistically significant association with long stay (Table 4).
DiscussionThis study allowed us to characterize the morbidity profile in preterm infants in NICUs in Northern Minas Gerais, revealing that respiratory and infectious conditions comprise the most common complications. It was also observed that there is still a significant association between frequency of these problems and gestational age, in an inverse relationship. These findings are consistent with the literature.
4,7,13,19,20Both national and international literature report that respiratory disorders are the main morbidity in NICUs, followed by infectious conditions. They also point to the occurrence of cardiac and metabolic problems.
4,7,11 Bronchopulmonary dysplasia, intracranial hemorrhage and necrotizing enterocolitis,
7 are also highlighted and were likewise observed in this study. The results of this study point to a statistically significant association between the main morbidities observed and the classification of gestational age. Distinct data were recorded in China,
7 where the authors observed a higher occurrence of some complications in moderate preterm infants (between 29 and 32 weeks). In that study, this finding is justified by the high number of preterm infants discharged without medical authorization, within few days after birth, at the request of the families – a situation that is not recorded in Brazil.
In a cohort study conducted across 25 hospitals in the United States, the authors highlighted the occurrence of complications such as ICH, seizures, necrotizing enterocolitis, bronchopulmonary dysplasia, and respiratory distress. They also stated that the frequency of all morbidities reduces significantly after 32 weeks of gestational age.
21The identification and recognition of the main morbidities that affect preterm neonates is significant, considering that some of those are avoidable and adequate and timely treatment may favorably interfere in the future life of these children. In a study conducted in Israel, the authors assessed the impact of the most frequent neonatal morbidities related to postnatal growth, recording that respiratory distress syndrome, bronchopulmonary dysplasia, necrotizing enterocolitis, patent ductus arteriosus and intraventricular hemorrhage are common conditions for neonates with birthweight under 1500g and interfere significantly with the extrauterine growth.
20 A follow-up study conducted in the United States concluded that preterm neonates that survived conditions such as necrotizing enterocolitis, sepsis, ICH and bronchopulmonary dysplasia had high rates of readmissions and neuropsychomotor delays.
19Regarding the factors associated with long NICU stays, this study revealed that lower gestational age, lower birthweight, late-onset sepsis and necrotizing enterocolitis are intimately associated with longer hospital stay, highlighting that the aspects related to the care provided to preterm infants interfere with the length of NICU stay, besides prematurity itself. In light of these findings, it is worth highlighting that the literature does not define a maximum length for NICU stay, nor does it define what constitutes a long stay for preterm neonates. In Brazil, particularly, few studies approach the length of hospitalization in the neonatal period.
4,22,23In two systematic reviews on the subject,
9,10 the authors highlight the significance of standardizing concepts, especially given the increase of neonatal survival in the last years. This factor implies a broader usage of neonatal care in the long term, and consequently an increase in the total number of days of healthcare. In some of the studies identified, the length of hospitalization was measured since the postmenstrual age, and the researchers define it as late discharge when it occurs after 42 weeks of gestational age. In other studies, long hospital stay is defined as 21 days or more, in yet other studies, after the final quartile of the hospitalization period.
9,10 In this study, we opted to use the last quartile, assuming it as a condition that establishes the comparison between the care and the local conditions for all preterm infants.
A study that assessed perinatal and postnatal factors that influence the length of hospitalization in preterm NBs (25-33 weeks of pregnancy) admitted in NICUs in India, concluded that the length of hospitalization was increased in nine days per each week of pregnancy below the common period for pregnancy, as well as the increase of the length of hospitalization due to the presence of morbidities such as respiratory distress syndrome, bronchopulmonary dysplasia and sepsis.
24 A study from the United States concluded that the length of neonatal hospitalization decreased significantly with each entire week of pregnancy. For infants born between 26 and 32 weeks of gestation, each additional week in the womb reduced the subsequent length of neonatal hospitalization by at least eight days.
21In the present study, both gestational age and birthweight were independently associated with higher length of hospitalization. Although birthweight is a more objective measure than gestational age, it is influenced by factors that result in intrauterine growth restriction, with significant influence of the social conditions.
25 The prolonged hospital stay due to low birthweight is related to the dynamics of weight gaining itself. This is characterized by an initial weight loss, followed by the recovery of the birthweight, the intensity and length of these two stages inversely related to gestational age, birthweight and complications experienced by the neonate. This characteristic prevents the preterm NB from quickly reaching the necessary parameters for hospital discharge, thus resulting in prolonged hospital stay.
It is worth emphasizing that preterm NBs and/or those with low weight has determined conditions and are more vulnerable to determined morbidities, and accordingly, will require treatments and assistance with invasive or non-invasive techniques, the use of medication for the control of frequent homeostasis and phlebotomy and, all of these aspects will result in prolonged hospital stay. A study conducted in Minas Gerais also reported that the combination of lower birthweight and gestational age was associated with higher risk of prolonged hospital stay compared to other profiles of associated complications.
26In this study, although all clinical complications assessed were associated with a prolonged stay in the bivariate analyses, only two conditions remained statistically associated with a prolonged stay in the final model: late-onset sepsis and necrotizing enterocolitis. Both are severe and common clinical conditions for preterm infants, carrying a high risk of mortality.
27 The role of infection and feeding disorders (which may indicate necrotizing enterocolitis), was previously observed in other studies.
4,28 In that regard, the prevention of perinatal and nosocomial infection and the adoption of adequate and tolerable feeding strategies may be highly effective in the reduction of the length of NICU stay for low birthweight preterm infants.
NEC, in spite of the improvements in neonatal care, is still affecting approximately 7% of preterm infants with a birthweight lower than 1500 grams.
29 Its occurrence is associated with hypoxia and mesenteric ischemia, as a correlation of factors related to enteral feeding, gut microbiota and inflammation. One of the first events that leads to NEC is an abnormal response of the premature intestine to colonizing microorganisms. The inflammatory response, with mucosal lesions and bacterial translocation, defines a severe condition that requires prolonged care, thereby justifying a longer NICU stay.
29Neonatal sepsis is a frequent case of neonatal morbidity and mortality, mainly in developing countries. It is hard to diagnose, since its clinical signs are unspecific and supplementary exams have low accuracy.
30 The association of late-onset sepsis and BPD is particularly present in those cases in which sepsis is related to the need for mechanical ventilation for a prolonged period.
The variables related to neonatal morbidities that increase the length of stay highlight the need for constant surveillance in relation to care and management of preterm neonates in the NICUs. The possibility of treatment and repeated treatments for the recovery of preterm neonates with late-onset sepsis or NEC inherently leads to a prolonged hospital stay. This is initially due to the period necessary for antimicrobial administration and observation for potential resistance, and subsequently, to the time required for the health condition to evolve in response to the adopted treatment.
30 In that regard, the management of neonatal infectious processes remains a challenge that requires continuous surveillance of their risk factors and etiologic agents, which in turn facilitates improved care.
The findings of this study should be considered in the light of some limitations. It should be considered that the data refer to surviving neonates receiving care in a follow-up outpatient clinic. In that regard, data collected longitudinally, since the birth, would be more adequate for the definition of prolonged stays and its associated factors. It should be also considered the lack of standardization of the definition of prolonged stay in the literature. Demographic and social data related to the mothers and pregnancy conditions were not assessed as well, and they could add significant information to the results. It is also applied to the classification of severity for the clinical conditions assessed, which were not defined during data collection. In spite of its limitations, this study provides a panorama of hospital morbidity for neonates discharged from NICUs in Northern Minas Gerais, offering previously unknown data, and novel insights into prolonged hospital stay for the group evaluated. This highlights the need for broader surveillance and improved prenatal and postnatal care.
In conclusion, the factors associated with prolonged stay are primarily linked to the early interruption of gestations and neonatal care. This highlights the need for greater attention to prenatal care, including comprehensive follow-up prematurity prevention, as well as to postnatal care, with a greater focus on preventing nosocomial infections.
References1. World Health Organization (WHO). Born too soon: decade of action on preterm birth. Geneva: WHO; 2023. [
Internet] [access in 2024 Set 15]. Available from:
https://www.who.int/publications/i/item/97892400738902. Helenius K, Sjörs G, Shah PS, Modi N, Reichman B, Morisaki N,
et al; International Network for Evaluating Outcomes (iNeo) of Neonates. Survival in Very Preterm Infants: An International Comparison of 10 National Neonatal Networks. Pediatrics. 2017; 140 (6): e20171264.
3. Pravia CI, Benny M. Long-term consequences of prematurity. Cleve Clin J Med. 2020; 87 (12): 759-67.
4. Sousa DS, Sousa AS, Santos ADR, Melo EV, Lima SO, Almeida-Santos MA,
et al. Morbidity in extreme low birth weight newborns hospitalized in a high risk public maternity. Rev Bras Saúde Matern Infant. 2017; 17 (1): 149-57.
5. Sexty RE, van der Pal S, Reijneveld SA, Wolke D, Lüchters G, Bakker L,
et al. Changes in neonatal morbidity, neonatal care practices, and length of hospital stay of surviving infants born very preterm in the Netherlands in the 1980s and in the 2000s: a comparison analysis with identical characteristics definitions. BMC Pediatr. 2023; 23 (1): 554.
6. Lipner HS, Huron RF. Developmental and interprofessional care of the preterm infant: neonatal intensive care unit through high-risk infant follow-up. Pediatric Clinics. 2018; 65 (1): 135-41.
7. Cao Y, Jiang S, Sun J, Hei M, Wang L, Zhang H,
et al. Chinese Neonatal Network. Assessment of Neonatal Intensive Care Unit Practices, Morbidity, and Mortality Among Very Preterm Infants in China. JAMA Netw Open. 2021; 4 (8): e2118904.
8. Freitas Md, Kernkraut AM, Guerrero SM, Akopian ST, Murakami SH, Madaschi V,
et al. Follow-up of premature children with high risk for growth and development delay: a multiprofessional assessment. Einstein. 2010; 8 (2): 180-6.
9. Seaton SE, Barker L, Jenkins D, Draper ES, Abrams KR, Manktelow BN. What factors predict length of stay in a neonatal unit: a systematic review. BMJ Open. 2016; 6 (10): e010466.
10. Fu M, Song W, Yu G, Yu Y, Yang Q. Risk factors for length of NICU stay of newborns: A systematic review. Front Pediatr. 2023; 11: 1121406.
11. Santos J, Pearce SE, Stroustrup A. Impact of hospital-based environmental exposures on neurodevelopmental outcomes of preterm infants. Curr Opin Pediatr. 2015; 27 (2): 254-60.
12. Araki S, Saito T, Ichikawa S, Saito K, Takada T, Noguchi S,
et al. Family-centered care in neonatal intensive care units: combining intensive care and family support. J UOEH. 2017; 39 (3): 235-40.
13. Eze P, Al-Maktari F, Alshehari AH, Lawani LO. Morbidities & outcomes of a neonatal intensive care unit in a complex humanitarian conflict setting, Hajjah Yemen: 2017-2018. Confl Health. 2020; 14: 53.
14. Walter SD, Eliasziw M, Donner A. Sample size and optimal designs for reliability studies. Stat Med. 1998; 17 (1): 101-10.
15. Linhares MBM, Carvalho AEV, Bordin MBM, Chimello JT, Martinez FE, Jorge SM. Prematuridade e muito baixo peso como fatores de risco ao desenvolvimento da criança. Paidéia (Ribeirão Preto). 2000; 10 (18): 60-9.
16. Camargo VC, Silva SH, Nohama P, Amorim MF. Desenvolvimento de uma tecnologia para a detecção e interrupção do episódio da apneia da prematuridade. Texto Contexto Enferm. 2009; 18 (3): 449-57.
17. Ibrahim J, Bhandari V. The definition of bronchopulmonary dysplasia: an evolving dilemma. Pediatr Res. 2018; 84: 586-8.
18. Fleischmann-Struzek C, Goldfarb DM, Schlattmann P, Schlapbach LJ, Reinhart K, Kissoon N. The Global Burden of Paediatric and Neonatal Sepsis: A Systematic Review. Lancet Respir Med. 2018; 6: 223-30.
19. Bell EF, Hintz SR, Hansen NI, Bann CM, Wyckoff MH, DeMauro SB,
et al. Mortality, In-Hospital Morbidity, Care Practices, and 2-Year Outcomes for Extremely Preterm Infants in the US, 2013-2018. JAMA. 2022; 327 (3): 248-63.
20. OfekShlomai N, Reichman B, Zaslavsky-Paltiel I, Lerner-Geva L, Eventov-Friedman S; Israel Neonatal Network. Neonatal morbidities and postnatal growth failure in very low birth weight, very preterm infants. Acta Paediatr. 2022; 111 (8): 1536-45.
21. Manuck TA, Rice MM, Bailit JL, Grobman WA, Reddy UM, Wapner RJ,
et al. Preterm neonatal morbidity and mortality by gestational age: a contemporary cohort. Am J Obstet Gynecol. 2016; 215 (1): 103.e1-103.e14.
22. Quaresma ME, Almeida AC, Méio MDB, Lopes JMA, Peixoto MVM. Factors associated with hospitalization during neonatal period. J Pediatr. 2018; 94 (4): 390-8.
23. Moura BLA, Alencar GP, Silva ZP, Almeida MF. Fatores associados à internação e à mortalidade neonatal em uma coorte de recém-nascidos do Sistema Único de Saúde, no município de São Paulo. Rev Bras Epidemiol. 2020; 23: e200088.
24. Murki S, Vardhelli V, Deshabhotla S, Sharma D, Pawale D, Kulkarni D,
et al. Predictors of length of hospital stay among preterm infants admitted to neonatal intensive care unit: Data from a multicentre collaborative network from India (INNC: Indian National Neonatal Collaborative). J Paediatr Child Health. 2020; 56 (10): 1584-9.
25. Girma S, Fikadu T, Agdew E, Haftu D, Gedamu G, Dewana Z,
et al. Factors associated with low birthweight among newborns delivered at public health facilities of Nekemte town, West Ethiopia: a case control study. BMC Pregnancy Childbirth. 2019; 19 (1): 220.
26. Lima MDO, Silva TPR, Carmo AS, Mateus LMA, Marcatto JO, Matozinhos FP,
et al. Association between birth weight, gestational age and secondary diagnoses in the hospital stay of premature newborns. Rev Min Enferm. 2022; 26: e-1427.
27. Tomo CK, Balogunb OO, Davidson J, Guinsburg R, Almeida MFB, Lopes JMA,
et al. Comparison of mortality and survival without major morbidities of very preterm infants with very low birth weight from Japan and Brazil. Rev Paul Pediatr. 2023; 41: e2021389.
28. Niknajad A, Ghojazadeh M, Sattarzadeh N, Bashar Hashemi F, Shahgholi DKF. Factors affecting the neonatal intensive care unit stay duration in very low birth weight premature infants. J Caring Sci. 2012; 1 (2): 85-92.
29. Hackam D, Caplan M. Necrotizing enterocolitis: Pathophysiology from a historical context. SeminPediatr Surg. 2018; 27 (1): 11-8.
30. Procianoy RS, Silveira RC. The challenges of neonatal sepse management. J Pediatr. 2020; 96 (Suppl 1): 80-6.
Authors' contribution: Menezes MSD and Caldeira AP: idealization and coordination of the research project. Rodrighes JES and Mendonça IP: data analysis and collection. All authors equally contributed to the data analysis, writing and critical review of the manuscript. They approved the final version of the article and declared no conflicts of interest.
Data availability: All datasets supporting the results of this study are included in the article.
Received on September 11, 2024
Final version presented on July 19, 2025
Approved on July 21, 2025
Associated Editor: Karla Bomfim


 ; Jady Emanuelle Santos Rodrigues2
; Jady Emanuelle Santos Rodrigues2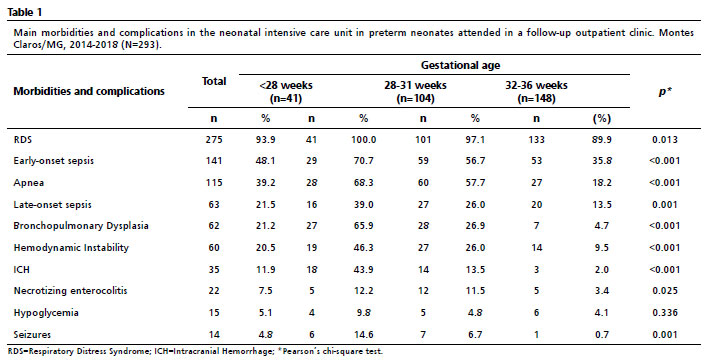






 Ler em português
Ler em português