ABSTRACT
OBJECTIVES: the first five years of life are critical for children's physical and intellectual development. However, the under-five mortality rate in South Asia and ASEAN is relatively high, caused by complex etiologies. This paper identifies maternal high-risk fertility behaviors and healthcare services utilization and examines predictors of under-five mortality (U5M) in 7 Asian (South Asia - ASEAN) developing countries (Indonesia, Myanmar, Cambodia, Philippines, Bangladesh, Nepal, and Pakistan).
METHODS: a multivariate logistic regression model with a complex survey was used to examine predictors of U5M on the frequency of U5M adjusted for comorbidities.
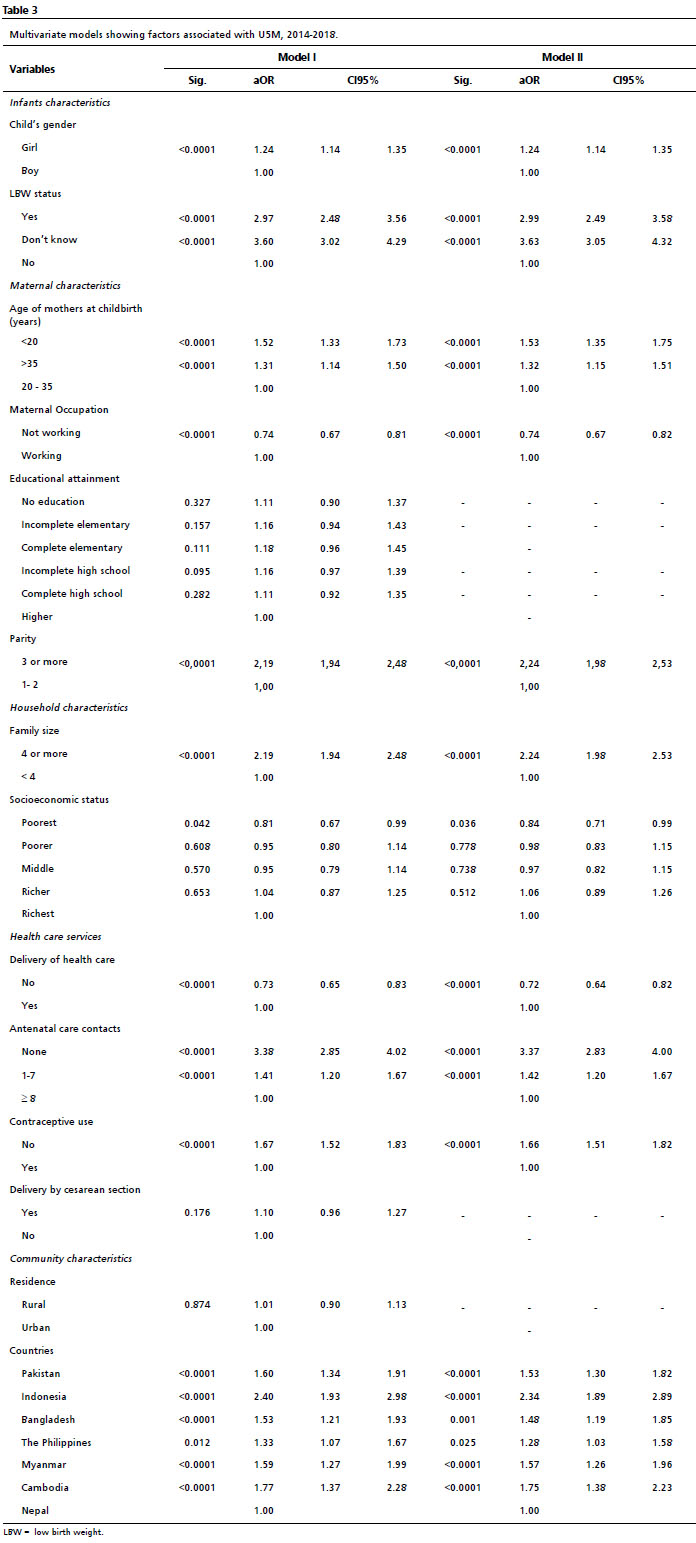
RESULTS: according to multivariate models (model 2), U5M was 2.99 times higher in mothers with low weight at birth infants than in mothers without low weight at birth infants (aOR= 2.99; CI95%=2.49-3.58); Mothers without antenatal care contacts were 3.37 times more likely (aOR= 3.37; CI95%=2.83-4.00) to have a U5M than mothers with eight or more antenatal care contacts; U5M in Indonesia was 2.34 times higher (aOR= 2.34; CI95%= 1.89-2.89). It is investigated that antenatal care serves as a predictor in decreasing U5MR.
CONCLUSIONS: in order to achieve significant U5MR reduction, intervention programs that encourage antenatal care consultations should be implemented.
Keywords:
Under-five mortality, Demographic health survey, Antenatal care
RESUMO
OBJETIVOS: os primeiros cinco anos de vida são críticos para o desenvolvimento físico e intelectual da criança. No entanto, a taxa de mortalidade de menores de cinco anos no sul da Ásia e na ASEAN é relativamente alta, causada por etiologias complexas. Este artigo identifica comportamentos maternos de fertilidade de alto risco e utilização de serviços de saúde e examina preditores de mortalidade abaixo de 5 anos (MM5) em 7 países em desenvolvimento da Ásia (Sul da Ásia - ASEAN) (Indonésia, Mianmar, Camboja, Filipinas, Bangladesh, Nepal e Paquistão).
MÉTODOS: um modelo de regressão logística multivariada foi usado para examinar preditores de MM5 na frequência de MM5 ajustado para comorbidades.
RESULTADOS: na análise multivariada (modelo 2), U5M foi 2,99 vezes maior em mães com bebês com baixo peso ao nascer do que em mães sem bebês com baixo peso ao nascer (aOR= 2,99; IC95%=2,49-3,58); as mães sem contatos de cuidados pré-natais tiveram 3,37 vezes mais probabilidade (aOR= 3,37; IC95%=2,83-4,00) para ter MM5 do que mães com oito ou mais contatos de cuidados pré-natais; MM5 na Indonésia foi 2,34 vezes maior (aOR= 2,34; IC95%= 1,89-2,89). Investiga-se que os cuidados pré-natais funcionam como um preditor na diminuição da MM5.
CONCLUSÕES: para uma redução significativa da MM5, devem ser implementados programas de intervenção que estimulem as consultas pré-natais.
Palavras-chave:
Mortalidade de menores de cinco anos, Pesquisa demográfica de saúde, Cuidado pré-natal
IntroductionUnder-five mortality (U5M) is a term that refers to a child's death before reaching the age of 5 years old.
1 The first five years of life are critical for children's physical and intellectual development.
2 Child mortality rates are the leading indicators of population health and well-being. Many used it to determine population health and trends, including neonatal and post-neonatal, infant, child, and under-five mortality rates (U5MR).
3Globally, remarkable progress has been made in lowering child mortality, especially for children under five. In 2018, there were 5.3 million fewer deaths among children under five compared to an estimated 12.6 million in 1990. A total of 2.5 million (47%) deaths occurred in the first month of life, 1.5 million (29%) deaths happened between 1-11 months of age, and 1.3 million (25%) deaths occurred between 1-4 years of age.
4The U5M rate is still relatively high in South Asia, with a 15-year prevalence (1999-2014) of 100 deaths per 1,000 births. In 2015, the World Bank reported 53 deaths among children under-five in South Asia.
5 Neonatal (the first 28 days of life) and infant (first year) deaths contribute to most deaths among children under five, and the highest child death rates in the world are found in South Asia countries. Three out of ten child deaths worldwide happen in South Asia.
6In 2010, around 7.6 million children worldwide under five died.
1 Access to affordable interventions could prevent or treat over two-thirds of these early child fatalities. Pneumonia, diarrhea, malaria, and infant health complications are among the top five causes of death in children younger than five years old. Malnutrition contributes to more than a third of all child fatalities.
7 The probability of dying before five for children in low-income nations is roughly 18 times higher than in high-income countries. Child mortality has been affected by numerous variables, and among these variables, poverty is regarded as the most significant cause of world's child mortality.
8Most recent child deaths occur in South Asian countries, where the rates are 42.1% and 25.8% for U5M and neonatal mortality, respectively. After successfully implementing the Millennium Development Goals (MDG), the U5M rate in Bangladesh dropped dramatically, from 133 to 30.2 deaths per 1000 live births between 1990 and 2018. Bangladesh's rate is lower than Pakistan's (69.3 per 1000 live births) but still higher than the rest of South Asia (36.6 per 1000 live births).
9Over the last 30 years, ASEAN (Association of Southeast Asian Nations) - Indonesia, Malaysia, Singapura, Thailand, Philippines, Brunei Darussalam, Vietnam, Laos, Myanmar, and Cambodia, has seen significant neonatal and infant survival gains. Child deaths in the first 28 days of life (neonatal mortality) and U5M have been significantly reduced across the ASEAN region, with Thailand and Singapore reducing neonatal mortality by around 75% and Thailand reducing infant mortality in a similar proportion. ASEAN member countries have the triple challenge of lowering infant mortality, mother and child mortality, and maternal mortality. High infant mortality rates imply poor maternal and child health services, particularly during and after birth.
10Between 1980 and 2015, the U5MR in Indonesia fell from 85.4 to 22.2, the highest reported drop among ASEAN members. Indonesia had the greatest U5MR among the five ASEAN countries, followed by the Philippines.
11 According to Nguyen,
12 the drop in infant mortality rate is not quick enough for most Asian sub-regions, including Southeast Asia. The primary causes of child fatalities in ASEAN, in particular, are avoidable illnesses like diarrhea and pneumonia. Furthermore, it has been observed that neonatal (first month of life) infant mortality is increasing compared to children deaths in later childhood.
In developing nations, U5MR is brought on by complicated etiologies such as premature birth, suffocation, sepsis, injuries, measles, respiratory infection, and congenital disease. It is critical to note that the majority of child deaths are the result of maternal factors that can be avoided during pregnancy, such as illnesses that can be transmitted via the intrauterine pathway into the fetus' blood flow.
13A recent study conducted by Tai
et al.
14 using the 2015-16 Myanmar Demographic Health Survey showed that there is an increased risk of death in children under-5 if antenatal care services which include skilled birth assistance, antenatal care, postnatal care, and tetanus vaccine are not used. Talukder
et al. ,
15 which conducted a study in Bangladesh, also stated that utilization of antenatal care services throughout pregnancy would unquestionably minimize the likelihood of child malnutrition and mortality, as well as maternal mortality and morbidity. Pregnancy problems can be detected at an early stage through antenatal care visits.
16 Meanwhile, medical experts can take action to stop or control potentially fatal bleeding or refer the patient to more advanced care if necessary. Babies have a better chance of survival if they are born in a facility with access to competent birth attendants and prenatal care.
17Various socioeconomic variables, maternal and child-related factors, and health service utilization factors, such as household wealth status; educational level of the mother; older maternal age; use of polluting fuel; higher parity; lack of antenatal care (ANC) visits; lack of skilled birth attendance; use of antenatal iron and folic acid (IFA) supplementation; and tetanus toxoid (TT) vaccination during pregnancy, were identified as major factors associated with childhood mortality.
18 In addition, other studies have highlighted the importance of variables at both community and individual levels for the survival of children. For a more accurate estimate and beneficial epidemiological understanding, these studies suggest incorporating variables at the community level.
19This study identifies maternal high-risk fertility behaviors effects and healthcare services utilization. It examines the predictor of U5M in 7 Asian (South Asia and ASEAN) developing countries.
MethodsThis cross-sectional study used secondary data from Demographic and Health Surveys (DHS) (2014-2018) (freely available to the public) to determine the primary predictor of U5M. The DHS is a nationally representative survey conducted every five years in low- and middle-income countries. This paper focused on seven countries with recent DHS data to evaluate mortality predictors for children under five years. Countries were included if they provided complete data on all variables and had current DHS data (2014-2018). The included nations were South Asian and ASEAN countries; Indonesia, Myanmar, Cambodia, Philippines, Bangladesh, Nepal, and Pakistan. The multivariate logistic regression model was used to examine the predictor of U5M on the occurrence of U5M adjusting with confounders.
The study's population consisted of women aged 15 to 49 who had given birth within the prior five years. Eligibility criteria of women were excluded from the analysis if the information on maternal and infants was missing. Following DHS procedures, weightings were applied to achieve objective values. The absence of weights can cause results to be biased toward the oversampled subpopulations. Therefore, the study sample comprised a weighted sample of 66,405 women. The DHS sample technique and data collection procedures are described elsewhere.
Study variables included health care services (i.e. , delivery of health care, ANC visits, contraceptive use, and delivery by cesarean section), Infants' characteristics (i.e. , gender and status of low birth weight - LBW); LBW status was defined as a birth weight of less than 2500 g. Maternal characteristics (i.e. , age of mothers at childbirth, maternal occupation, educational attainment, and parity). Household characteristics (i.e. , family size and socioeconomic status); the socioeconomic status of families was assessed by assessing the yearly household expenditures. Socioeconomic status was classified into five categories using quintiles. Based on information about household assets, asset wealth indices, which are constructed using principal component analysis, provide data on economic status. According to the results, the poor were categorized into the two lowest quintiles, while the highly wealthy were classified into the highest quintile. The survey also provides varieties of home (urban or rural) and regional (south Asian and ASEAN developing countries). The authors are interested in U5M as an outcome variable. Based on the definition of U5M (child will die before reaching five years of age), children were categorized as either under-five mortalities (Yes, coded 0) or non-under-five mortalities (No, coded 1).
The ethical practices were the responsibility of the organizations that sponsored, funded, or managed the surveys. Intermediate Care Facilities (ICF) International approves all DHS surveys and an Institutional Review Board (IRB) in the respective country to ensure that the protocols adhere to the US Department of Health and Human Services regulations for human subject protection.
The analyses were conducted with SPSS Version 28 licensed by Faculty of Public Health, Universitas Muhammadiyah Jakarta. All analyses adjusted for the complex survey design structure (clustering, weighting, and stratification). Descriptive statistics were computed for the independent and outcome variables. The authors combined the datasets of whole countries to produce a single dataset, resulting in a sample size of 66,640 women aged 15 to 49. The sample was stratified by country: Bangladesh (8,756), Pakistan (12,690), Nepal (5,038), Myanmar (4,784), Cambodia (7,126), the Philippines (10,530), and Indonesia (17,716). Using multivariate logistic regression models, factors related with U5M in South Asian and ASEAN developing countries were investigated. The regression analysis findings were provided as adjusted odds ratios (aOR) with 95% confidence intervals (CI), indicating statistical significance. The authors calculate U5M rate per country using the live birth as denominator.
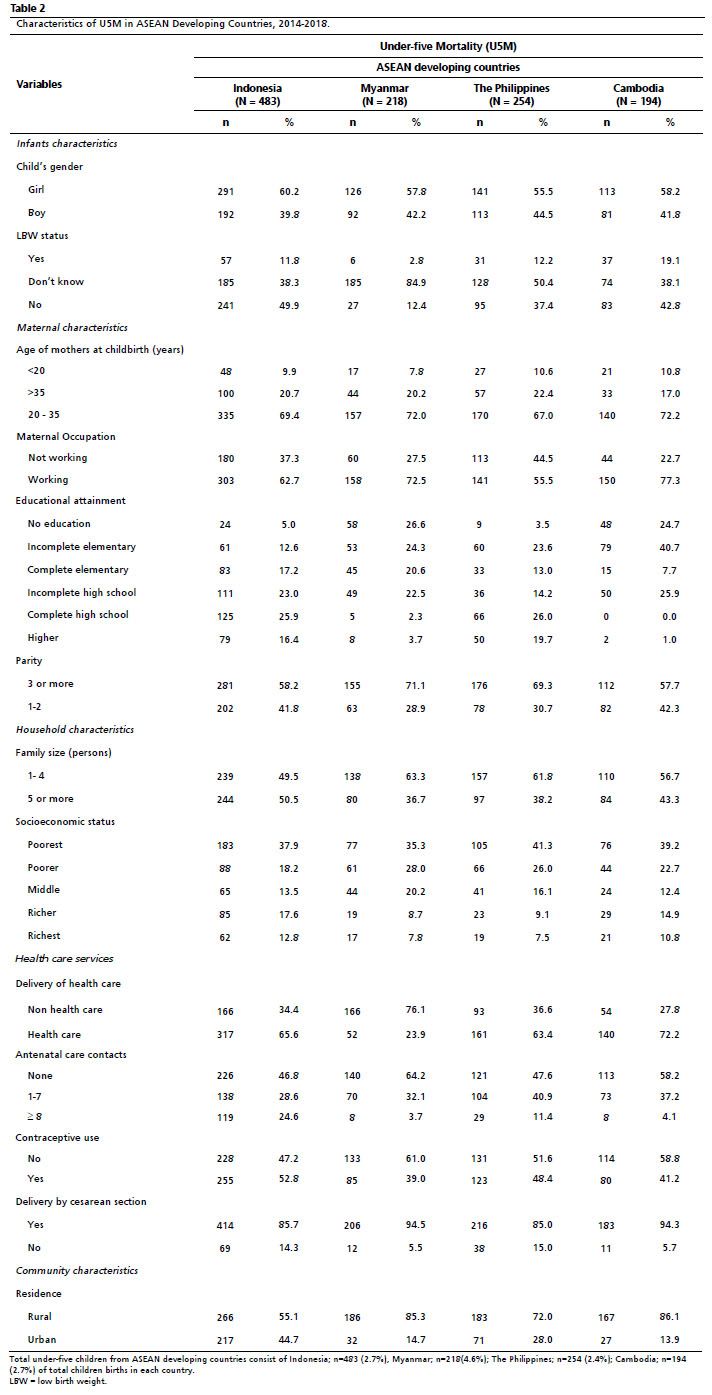
ResultsTables 1 and 2 show U5M characteristics among mother-child pairs, and the study included 66,640 mother-child pairs from South Asian and ASEAN developing countries. In seven countries, most U5M (46.2%-72.3%) were born to mothers with three or more children. Mothers who were not contacted by an antenatal care provider during their pregnancy had a 47.6%-70.93% U5MR. 75.4-96.0 % of U5M occurred via cesarean section. The Philippines and Indonesia are the only countries with a high proportion of secondary school graduates (25.9%-26.0%), while other countries have a high proportion of low-level secondary school graduates. The majority were from rural areas (86.1%-48.6%). Based on total children born in each country, the majority of U5M was seen in South Asia; Pakistan (5.7%), Bangladesh (4.1%), Nepal (3.5%); and ASEAN countries; Myanmar (4.6%), Indonesia (2.7%), Cambodia (2.7%), and The Philippines (2.4%).
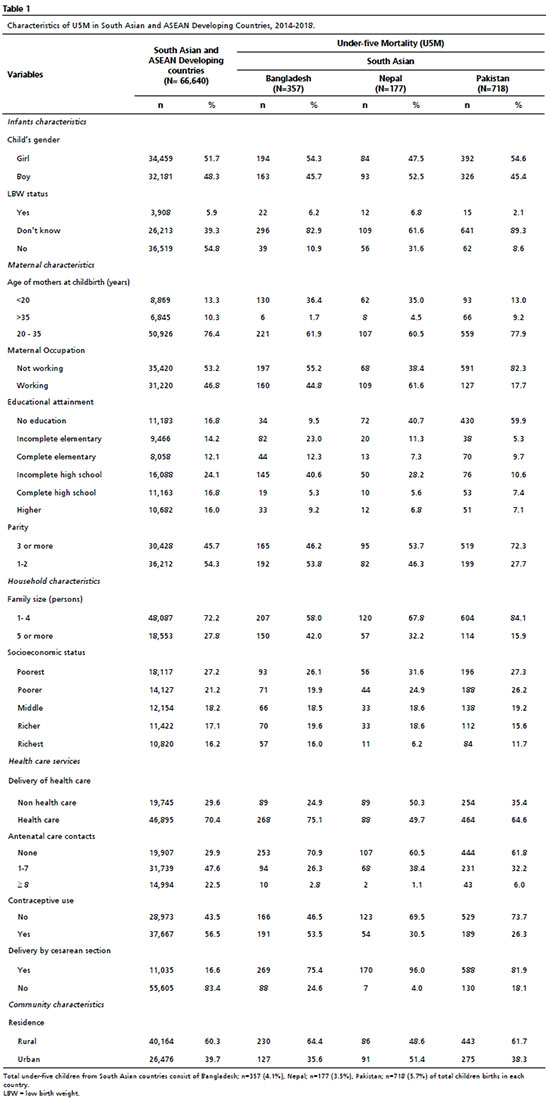
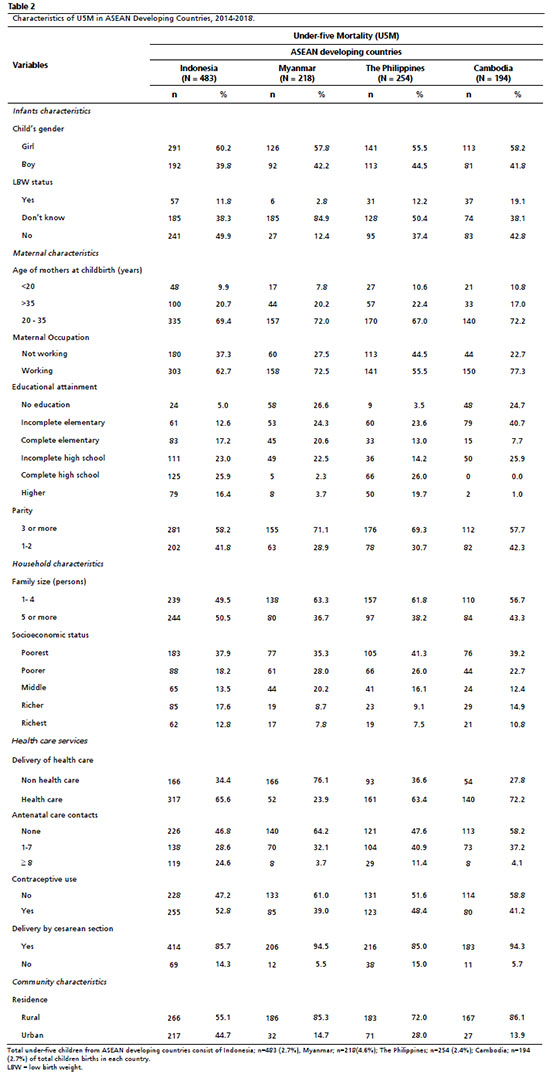
Table 3 includes all of the characteristics that have been identified as essential determinants of U5M in various studies. All aspects shown in Table 2 were included in the multiple regression analysis in the pooled data (Model 1; Model 2). Although socioeconomic status, cesarean delivery, and type of residence are not statistically significant, their effects are associated with U5M once other variables in the conceptual framework are controlled for, such as the survey indicator. According to multivariate models (model 2), girls are 1.24 times more likely to experience U5M than boys (aOR= 1.24; CI95%= 1.14-1.35). Children with LBW were 2.99 times more likely to experience U5M than normal weight birth (aOR= 2.99; CI95%= 2.49-3.58;
p<0.0001). Mothers whose age was less than 20 years had a significantly higher experience U5M than mothers from the age group 20-35 years (aOR=1.53, CI95%= 1.35-1.75;
p<0.0001). Mothers with parity 3+ (three or more) were 2.24 more likely to experience U5M than mothers who had parity 1-2. Mothers without ANC contacts were 3.37 times more likely (aOR= 3.37; CI95%=2.83-4.00) to have U5M than mothers with eight or more ANC contacts. U5M was 2.99 times higher in mothers with LBW infants than in mothers without LBW infants (aOR= 2.99; CI95%=2.49-3.58). U5M in Indonesia was 2.34 times higher (aOR=2.34; CI95%= 1.89-2.89) compared with Nepal.
DiscussionChildren with second or third birth order (OR = 1.316; CI95%=1.097-2.343), fourth or fifth birth order (OR = 1.934; CI95%=1.678- 3.822), and sixth or above birth order (OR = 3.980; CI95%=2.352-6.734) were significantly associated with increased risk of under-five mortality relative to those with first birth order.
20 This agrees with the findings of the previous investigation. Children with a higher birth order had a higher risk of under-five mortality than those with a lower birth order.
21,22 The reason for this might be that given the number of children a mother has, the care she provides to each child decreases. It was discovered that children from larger families were more likely to pass away before the age of 5 than those from smaller families.
20This aligns with previous research findings by Gebretsadik and Gabreyohannes
23 which may be due to the fact that as the size of the family increases, the proportion of food and other limited resources necessary for child survival decreases. Multiple births were associated with an increased risk of infant mortality compared to single pregnancies. Possible explanations include the sharing of consumables and other limited resources, as well as the care provided by mothers to their children.
23,24The odds of U5M increased by 31% in children with low birth weight compared to children with normal birth weight.
22 This is similar to the findings of previous a previous research by Ahinkorah
et al. ,
25 which found that children who were very little at birth had a greater under-five mortality rate (207 deaths per 1,000 live births) than those who were larger than normal at birth (102 deaths per 1,000 live births).
According to Aheto's research in Ethiopia, female babies were 1.31 times more likely to die before reaching the age of five.
24 Newborn girls have a biological advantage in survival over newborn boys because they are less vulnerable to perinatal conditions (such as birth trauma, intrauterine hypoxia and birth asphyxia, prematurity, respiratory distress syndrome, and neonatal tetanus), congenital anomalies, and infectious diseases such as intestinal infections and lower respiratory infections. However, girls do not have the same advantage regarding some infectious diseases, which are the leading causes of death in later infancy and early childhood in environments with high general mortality. As a result, the sex ratio of child mortality is lower than the sex ratio of infant mortality. The sex ratio of under-five mortality is in the middle, and the relative mortality levels of the baby and child age groups determine it.
22Large family sizes have been linked to a decrease in child mortality. Families with seven or more members were 0.49 times (aOR = 0.49; CI95%= 0.29-0.80) or (51%), and families with four to six members were 0.65 times (aOR = 0.65; CI95%= 0.41-0.92) or (35%), less likely to have a child that dies than families with three or fewer members. It could be because when household members are prominent, mothers have more time to care for their children, lowering child mortality. However, from an economic standpoint, additional research is required because households with large family sizes need adequate access to essential requirements and services such as clean water, food, education, and health.
26Tagoe
et al.
27 discovered that compared to children of mothers who used a modern type of contraception, children of mothers who were non-users of contraception but expected to use it later were less likely to die before the age of five. There is a low incidence of modern contraceptive usage among reproductive-age women in Sierra Leone. Hence using modern contraceptives does not influence under-five mortality. Another possible explanation is that mothers, who are currently non-users but intend to use contraception later, may have had their ideal number of surviving children and may be making plans for childbirth control, which could explain why their children were less likely to die.
Using data from demographic health surveys among seven developing south Asian and ASEAN nations, the authors also investigated the impact of ANC visits on child health outcomes, specifically U5M mothers without ANC contacts were 3.37 times more likely to have a U5M than mothers with eight or more ANC contacts. U5M was 2.99 times higher in mothers with LBW infants than mothers without LBW infants. Our study also investigated that U5M in Indonesia was 2.34 times higher among 7 South Asia and ASEAN developing countries. It is in line with the report from World Health Organization (WHO) (2020) that Indonesia ranks seventh in the world and is the only Southeast Asian country that is included in the world ranking for U5M, with an anticipated 115 deaths in 2019, surpassing the United Republic of Tanzania, Angola, and Bangladesh.
Infant and child mortality risk factors include the number of ANC visits. Children born to mothers who had fewer than the required ANC visits were more likely to die than children born to women who had the recommended visits.
28 WHO advises at least eight contacts, including one in the first trimester, five in the third trimester, and two in the second trimester. ANC offers the opportunity to deliver information to pregnant women, manage existing social and medical issues, and check for risk factors.
This study aligns with several kinds of research conducted in low- and middle-income countries. Abir
et al.
29 conducted a cross-sectional study in Bangladesh using multivariate logistic regression to analyze three demographic health surveys and discovered that women who had ANC visits had a lower risk of U5M. Arunda
et al.
30 investigated the impact of antenatal care services on neonatal mortality in Kenya. Based on a binary logistic regression, their findings show that mothers who attended ANC visits had the lowest neonatal mortality rates.
30 Another study by Tai
et al. ,
14 using the Myanmar Demographic Health Survey 2015-16 found that children whose mothers used ANC facilities such as government hospitals, private hospitals, and mobile clinics had a considerably lower risk of mortality.
14Furthermore, compared to children whose mothers did not get ANC, those born to mothers who did have a lower chance of death. Despite being at odds with the findings of other studies, this one agrees with the Ethiopian study. Mothers who have ANC visits and other forms of maternal health care may be better able to protect their infants from illness by learning about proper feeding techniques and other preventative measures. In addition, mothers who go to ANC may be more likely to get postnatal care, which is crucial for early spotting health issues in children and acting on them effectively. ANC visits may be advantageous for both the infant and the mother. ANC is an opportunity to promote good behavior and parenting skills, which are especially crucial for new mothers.
In addition, ANC is a well-established process that helps to identify problems related to maternal morbidity and mortality through relevant physical examinations. Fewer issues connected to maternal health have occurred in those who have obtained a minimum number of ANC services from health professionals in various government and non-government facilities, resulting in a reduction in maternal morbidity and mortality.
This study is one of the first to investigate the risk factors of U5M in 7 developing south Asian and ASEAN nations, especially in Indonesia as the highest U5M. The U5MR of Indonesian children suggests a drop but still sluggish development despite the SDGs' additional measures.
The limitation of this study is the fact that the antenatal health care utilization in the DHS was self-reported. It may have been influenced by social desirability within the society where the women lived. Furthermore, ANC attendance was assessed for births that took place in the years prior to the study, which could have been affected by recall bias. The definition of ANC may vary from nation to country and may not always require treatment from trained health professionals, therefore the outcome should be assessed in this perspective. Since the data is cross-sectional, causal inference is constrained. Furthermore, authors may also wish to consider data on missing LBW. In addition to this, a significant portion of the children did not have their birth weight recorded. The current findings may be affected by such missing values.
The paper investigated that ANC functions as a predictor in decreasing U5MR. ANC visits on child health outcomes, specifically U5M mothers without ANC contacts, were 3.37 times more likely (aOR= 3.37; CI95%=2.83-4.00) to have a U5M than mothers with eight or more ANC contacts. Intervention initiatives that promote more prenatal care visits must be taken into consideration if the goal is to significantly lower the U5MR. It will increase child survival and contribute in achieving the aims of the Sustainable Development Goals.
References1. UNICEF, WHO, World Bank Group, United Nations. Levels & Trends in Child Mortality. Report 2018: Estimates developed by the UN Inter-agency Group for Child Mortality Estimation. New York: UNICEF; 2018. [access in 2022 Feb 6]. Available from:
https://www.unicef.org/media/47626/file/UN-IGME-Child-Mortality-Report-2018.pdf2. Worku MG, Teshale AB, Tesema GA. Determinants of under-five mortality in the high mortality regions of Ethiopia: mixed-effect logistic regression analysis. Arch Public Health. 2021; 79 (1): 1-9.
3. Karyani AK, Kazemi Z, Shaahmadi F, Arefi Z, Meshkani Z. The Main Determinants of Under-5 Mortality Rate (U5MR) in OECD Countries: A Cross-sectional Study. Int J Pediatr. 2015; 3 (14): 421-7.
4. UNICEF, WHO, World Bank Group, United Nations. Levels & Trends in Child Mortality. Report 2019: Estimates developed by the UN Inter-agency Group for Child Mortality Estimation. New York: UNICEF; 2019. [access in 2022 Feb 6]. Available from:
https://www.unicef.org/media/60561/file/UN-IGME-child-mortality-report-2019.pdf5. Fundo das Nações Unidas para a Infância (UNICEF). Reducing Newborn Mortality in South Asia : A Results-Based Management Approach to Improving Knowledge and Accelerating Results. Ásia do Sul: UNICEF; 2016. [access in 2022 Feb 6]. Available from:
https://www.unicef.org/rosa/media/721/file/UNICEF%20Newborn%20Strategy%202016.pdf6. Kannaujiya AK, Kumar K, Upadhyay AK, McDougal L, Raj A, James KS,
et al. Effect of preterm birth on early neonatal, late neonatal, and postneonatal mortality in India. PLOS Glob Public Health. 2022; 2 (6): 1-17.
7. Madewell ZJ, Whitney CG, Velaphi S, Mutevedzi P, Mahtab S, Madhi AS,
et al. Prioritizing Health Care Strategies to Reduce Childhood Mortality. JAMA Netw Open. 2022 Oct; 5 (10): e2237689.
8. Karlsson O, Kim R, Hasman A, Subramanian SV. Age Distribution of All-Cause Mortality Among Children Younger Than 5 Years in Low- and Middle-Income Countries. JAMA Netw Open. 2022 May; 5 (5): e2212692.
9. Khan MA, Khan N, Rahman O, Mustagir G, Hossain K, Islam R,
et al. Trends and projections of under-5 mortality in Bangladesh including the effects of maternal high-risk fertility behaviours and use of healthcare services. PLoS One. 2021 Feb; 16 (2): e0246210.
10. Sari VK, Prasetyani D. Socioeconomic Determinants of Infant Mortality Rate in ASEAN: a Panel Data Analysis. J ASEAN Stud. 2021; 9 (1): 73-85.
11. Subramaniam T, Loganathan N, Yerushalmi E, Devadason ES, Majid M. Determinants of Infant Mortality in Older ASEAN Economies. Soc Indic Res. 2016; 136 (1): 397-415.
12. Nguyen VD. Child mortality declines in Asia — just not quickly enough. [
Internet]. East Asia Forum: Economics, Politics and Public Policy in East Asia and the Pacific; May 2013. [access in 2022 Feb 6]. Available from:
https://www.eastasiaforum.org/2013/05/09/child-mortality-declines-in-asia-just-not-quickly-enough/#more-3558713. Aguilera X, Delgado I, Icaza G, Apablaza M, Villanueva L, Castillo-Laborde C. Under five and infant mortality in Chile (1990-2016): Trends, disparities, and causes of death. PLoS One. 2020 Sep; 15 (9): e0239974.
14. Tai N, Htut SHT, Swe T. Impact of Use of Health Care on Under-5 Child Mortality among States and Regions: Analysis of the 2015-16 Myanmar Demographic and Health Survey. DHS Working Papers. 2019; 147: 1-33. [access in 2022 Feb 6]. Available from:
https://dhsprogram.com/pubs/pdf/WP147/WP147.pdf15. Talukder A, Siddiquee T, Noshin N, Afroz M, Ahammed B, Halder HR. Utilization of antenatal care services in bangladesh: A cross-sectional study exploring the associated factors. Anatol J Fam Med. 2021; 4 (1): 49-56.
16. Moller AB, Petzold M, Chou D, Say L. Early antenatal care visit: a systematic analysis of regional and global levels and trends of coverage from 1990 to 2013. Lancet Glob Health. 2017 Oct; 5 (10): e977-83.
17. Gabrysch S, Nesbitt RC, Schoeps A, Hurt L, Soremekun S, Edmond K,
et al. Does facility birth reduce maternal and perinatal mortality in Brong Ahafo, Ghana? A secondary analysis using data on 119 244 pregnancies from two cluster-randomised controlled trials. Lancet Glob Health. 2019 Aug; 7 (8): e1074-87.
18. Naz S, Page A, Agho KE. Potential Impacts of Modifiable Behavioral and Environmental Exposures on Reducing Burden of Under-five Mortality Associated with Household Air Pollution in Nepal. Matern Child Health J. 2018; 22 (1): 59-70.
19. Adekanmbi VT, Kandala NB, Stranges S, Uthman OA. Contextual socioeconomic factors associated with childhood mortality in Nigeria: a multilevel analysis. J Epidemiol Community Health. 2015 Nov; 69 (11): 1102-8.
20. Gobebo G. Determinant Factors of Under-five Mortality in Southern Nations, Nationalities and People's region (SNNPR), Ethiopia. Ital J Pediatr. 2021; 47 (1): 1-9.
21. Woldeamanuel BT. Socioeconomic, Demographic, and Environmental Determinants of Under-5 Mortality in Ethiopia: Evidence from Ethiopian Demographic and Health Survey, 2016. Child Dev Res. 2019; 2019: 1-15.
22. Kayode GA, Adekanmbi VT, Uthman OA. Risk factors and a predictive model for under-five mortality in Nigeria: Evidence from Nigeria demographic and health survey. BMC Pregnancy Childbirth. 2012 Feb; 12: 10.
23. Gebretsadik S, Gabreyohannes E. Determinants of Under-Five Mortality in High Mortality Regions of Ethiopia: An Analysis of the 2011 Ethiopia Demographic and Health Survey Data. Int J Popul Res. 2016; 2016: 1-7.
24. Aheto JMK. Predictive model and determinants of under-five child mortality: Evidence from the 2014 Ghana demographic and health survey. BMC Public Health. 2019; 19 (1): 1-10.
25. Ahinkorah BO, Budu E, Seidu AA, Agbaglo E, Adu C, Osei D,
et al. Socio-economic and proximate determinants of under-five mortality in Guinea. PLoS One. 2022 May; 17 (5): e0267700.
26. Gebremichael SG, Fenta SM. Factors Associated with U5M in the Afar Region of Ethiopia. Adv Public Health. 2020; 2020: 1-9.
27. Tagoe ET, Agbadi P, Nakua EK, Duodu PA, Nutor JJ, Aheto JMK. A predictive model and socioeconomic and demographic determinants of under-five mortality in Sierra Leone. Heliyon. 2020 Mar; 6 (3): e03508.
28. Shobiye DM, Omotola A, Zhao Y, Zhang J, Ekawati FM, Shobiye HO. Infant mortality and risk factors in Nigeria in 2013−2017: A population-level study. EClinicalMedicine. 2022 Aug; 51: 101622.
29. Abir T, Ogbo FA, Stevens GJ, Page AN, Milton AH, Agho KE. The Impact of Antenatal Care, Iron-folic Acid Supplementation and Tetanus Toxoid Vaccination during Pregnancy on Child Mortality in Bangladesh. PLoS One. 2017 Nov; 12 (11): e0187090.
30. Arunda M, Emmelin A, Asamoah BO. Effectiveness of Antenatal Care Services in Reducing Neonatal Mortality in Kenya: Analysis of National Survey Data. Glob Health Action. 2017; 10 (1): 1328796.
Received on January 10, 2023
Final version presented on June 7, 2023
Approved on July 6, 2023
Associated Editor: Melânia Amorim
Authors' contribution: Hastono SP made a substantial contribution to the conception and design of the investigation, and writing of the article. Lusida N made a significant contribution to the study's conception, design, and data collection. Arinda YD, Arsyi M and Andriyani made major contributions to the manuscript's critical evaluation. Each author equally agreed to be responsible for all aspects of the work after reading and approving the final draft before it was released. All authors declare no conflicts of interest.


 ; Nurmalia Lusida2
; Nurmalia Lusida2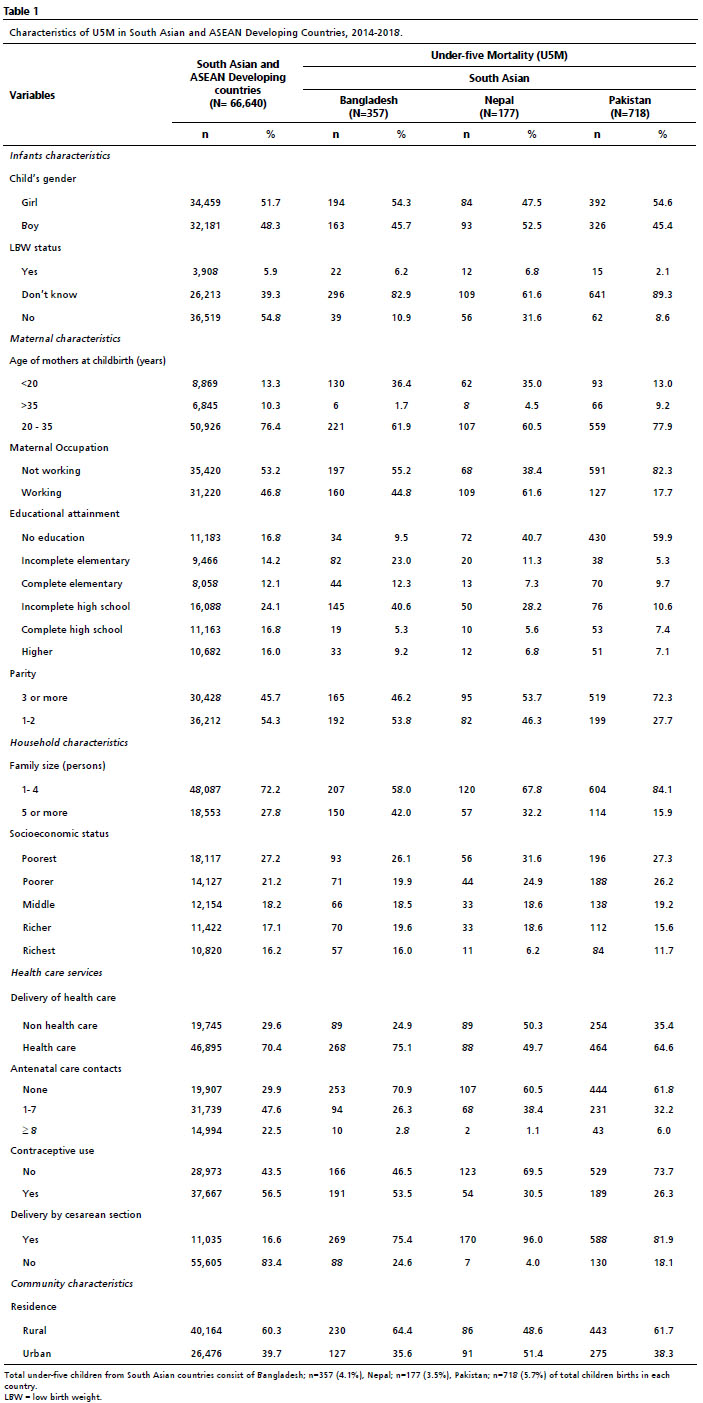






 Ler em português
Ler em português