ABSTRACT
OBJECTIVES: to analyze the relationship between parental practices, screen time, and food selectivity in children at 12 months of age.
METHODS: a cross-sectional study nested within a randomized clinical trial. In addition to sociodemographic information and the child's nutritional status, variables selected included the degree of food selectivity, parental practices (parent-centered practices/high control, parent-centered practices/contingency management, child-centered practices), obtained through validated questionnaires: The Child Eating Behavior Questionnaire and the Parental Feeding Style Questionnaire, as well as the use of electronics by children during meals. Crude and adjusted linear regression analysis were performed to assess the association between parental practices and food selectivity.
RESULTS: the use of parent-centered/contingency management practices were higher among female infants (p=0.034) and children classified as eutrophic (p=0.021). Parent-centered/high control practices and child-centered practices were positively associated with food selectivity (p=0.037 and p=0.048, respectively).
CONCLUSIONS: the evidence that parental feeding practices are associated with a child's food selectivity highlights the importance of initiatives aimed at providing appropriate guidance to parents during this stage of life.
Keywords:
Food fussiness, Feeding behavior, Child, Parent-child relations
RESUMO
OBJETIVOS: analisar a relação entre práticas parentais, uso de telas e a seletividade alimentar de crianças aos 12 meses de idade.
MÉTODOS: estudo transversal aninhado a um ensaio clínico randomizado. Foram selecionadas, além de variáveis de informações sociodemográficas e o estado nutricional da criança, o grau de seletividade alimentar, práticas parentais (práticas centradas nos pais/alto controle, práticas centradas nos pais/manejo de contingências, práticas centradas na criança), obtidas a partir de questionários validados: Child Eating Behavior Questionnaire e Questionário de Estilos Parentais na Alimentação, e uso de eletrônicos por crianças durante as refeições. Análise de regressão linear bruta e ajustada foi realizada para avaliação da associação entre as práticas parentais e a seletividade alimentar.
RESULTADOS: o uso de práticas centradas nos pais/manejo de contingências foi maior em lactentes do sexo feminino (p=0,034) e em crianças classificadas como eutróficas (p=0,021). As práticas centradas nos pais/alto controle e as práticas centradas na criança apresentaram associação positiva com a seletividade alimentar (p=0,037 e p=0,048, respectivamente).
CONCLUSÕES: a evidência de que as práticas parentais na alimentação estão associadas à seletividade alimentar da criança reforça a importância de iniciativas que visem a adequada orientação dos pais nessa fase da vida.
Palavras-chave:
Seletividade alimentar, Comportamento alimentar, Criança, Relações pais-filho
IntroductionFood fussiness is characterized by the refusal of a great variety of foods, familiar or new, and by determined food preferences, resulting in the intake of a low variety of food,
1,2 which can lead to dietary monotony and insufficient nutrient intake.
3 Children with this characteristic are still prone to consume a lesser amount of fruits and vegetables, as well as a higher amount of sweets.
2,4 In spite of being common during childhood, this behavior, in some cases, may persist beyond this stage, leading to consequences in growth and development of children, affecting their health in long-term.
5,6Several factors seem to be associated with food fussiness, both intrinsic and extrinsic ones, such as: genetics, higher sensibility to smells and textures, personality, maternal depression and anxiety, parental styles, parental practices and characteristics of the family environment.
1The parental food practices, that is, strategies conducted by parents to reach certain objectives for feeding their children, have an important role in the development of food preferences and in the eating behavior of children. Responsive food practices centered in children, which assure a pleasant and structured moment during meals, seem to be related to a positive eating behavior of these children. On the other hand, non-responsive food practices, centered on parents, that do not respect signs of hunger and satiety of children and do not allow them to have autonomy to make choices, seem to be associated with negative eating behaviors and food fussiness.
7,8Since food fussiness may lead to negative outcomes not only in children's growth and development, but also to the health of an individual, it is extremely important to understand factors associated with this behavior. Although food fussiness is being investigated in the scientific literature,
1,2,6,9,10 there are still gaps in knowledge concerning the impact of parental practices in the development of this behavior, mainly in children under two years of age. Thus, a more profound investigation of parental practices in this early childhood stage may bring knowledge to strategies that may prevent and manage this situation, promoting early a healthy and positive relationship with food. Given the above, the objective of this study is to analyze the relationship between parental practices, screen time and food fussiness in children at 12 months of age.
MethodsA nested cross-sectional study, contained within a randomized clinical trial (RCT) entitled "Methods of introduction of supplementary food in children: A randomized clinical trial". The RCT was performed with mother-nursling pairs, enrolled online in 2019 and followed-up until 2020, submitted to three different methods of healthy supplementary food (SF) introduction, based on three different methods: (A) Traditional; (B) Baby-Led Introduction to Solids (BLISS); and (C) Mixed method (combination between BLISS and traditional methods). Mothers participated in the intervention at five and a half months of life of the nursling, when they received guidance about exclusive breastfeeding, as well as the method of SF to which they were randomized. The subsequent questionnaires could be answered by any family member who participated in children feeding. Data from RCT protocol were published previously.
11For this study, we selected sociodemographic information, the nutritional status of children, the level of food fussiness, parental practices (parent-centered practices/high control, parent-centered practices/contingency management,child-centered practices) and screen time during meals.
The sociodemographic variables were collected by means of an online questionnaire sent to mothers. The tool contained questions about maternal schooling (with or without higher education), total family income (Brazilian real – the minimum wage was R$998.00 in the study period), maternal race/ethnicity (white or non-white – brown, black, yellow or indigenous), maternal marital status (with or without partner), nursling's gender (female or male) and number of children (multipara or primipara).
Anthropometric assessment was performed at 12 months of life of children by previously trained professionals. Weight and height of children were measured according to standardized anthropometric techniques. The anthropometric index "Body Mass Index" (BMI) -for-age (BMI/A) was calculated with the Anthro software of the World Health Organization (WHO).
12 The diagnosis of nutritional status was made following the reference curves, according to the technical standards of the Food and Nutrition Surveillance System (SISVAN – Portuguese acronym),
13 for each group of z-score of the BMI for age (BMI/A): extreme thinness (<z-score -3), thinness (≥ z-score -3 ≥ z-score -2), normality (≥ z-score -2 and ≥ z-score +1), risk of overweight (> z-score +1 and ≤ z-score +2), overweight (> z-score +2 and ≤ z-score +3), and obesity (> z-score +3). In order to perform analyzes, we opted to exclude the category "thinness", since it had only one participant, also to unify the categories "risk of overweight" and "overweight". Accordingly, the sample was divided into children with adequate BMI/Aand children with high BMI/A.
The subscale "Fussiness" in the adapted and validated to Portuguese version of the Child Eating Behavior Questionnaire (CEBQ) was used to assess the level of food fussiness of children in the study, observing that this is a tool used in studies that assess food fussiness in children.
1,2 The CEBQ was answered by the guardians at 12 months of age of the child, by means of a digital self-administered form.
The CEBQ was developed by Wardle et al.
14 in order to assess the eating behavior of children from two to seven years, from the subjective perception of parents or guardians. The questionnaire is composed of 35 items, divided into eight subscales: Satiety responsiveness, Slowness in eating, Food fussiness, Food responsiveness, Enjoyment of food, Desire to drink, Emotional overeating and Emotional undereating.
The subscale "food fussiness" is composed of six items: "my child enjoys tasting new foods"*, "my child enjoys a wide variety of foods"*, "my child is difficult to please with meals"*, "my child is interested in tasting food s/he hasn't tasted before"* "my child decides that s/he doesn't like a food, even without tasting it" and "my child refuses new foods at first". Each item was answered from a Likert scale of five points, which refer to the frequency with which the behavior occurs: "never", "seldom" , "sometimes", "frequently" and "always". The questions are scored from 1-5, except for the reverse questions (signaled with "*"), which are scored from 5-1. For data analysis, we then made a mean for the answers of the six items, the higher mean values indicating higher food fussiness.
The questionnaire was translated into Portuguese and validate by Viana and Sinde.
15 Moreover, although the validation is meant for the use in children from 36 months on, the tool was already used in children from 12 months on and the use in children younger than 36 months was validated in low- and middle-income countries.
16,17The parenting practices were assessed with the Parental Feeding Style Questionnaire (PFSQ).
18 The questionnaire was answered by the guardians at 12 months of age of the child with a digital self-administered form.
The PFSQ is the translated and adapted to Brazilian Portuguese version of the Caregiver's Feeding Style Questionnaire (CFSQ). The CFSQ was developed by Hughes et al.
19 To investigate the strategies used by parents during their children's meals. The translated version of the tool is composed of 19 items that should be answered from a 5 points Likert scale, scored similarly to the PFSQ.
We analyzed parenting practices: practices centered in parents/high control, practices centered in parents/ management of contingencies, practices centered in the child. The items centered in the child assess the promotion of his/her autonomy during a meal, and include practices such as making the feeding to become more ludic, talking about the benefits of foods, to compliment and make positive comments during the meals. The items centered on the parents, in turn, assess the external pressure used to control the feeding of their children. The practices centered in parents/high control are practices that use physical strength and pressure for encouraging children to eat; the practices centered in parents/management of contingencies include the use of rewards – the latter being foods or not – and the use of blackmail.
For the analysis of practices centered in parents/high control, we performed the mean of items 1, 16 and 19 from the questionnaire; for the practices centered in parents/management of contingencies, we performed the mean of items 2, 12, 18 and 14; for the analysis of practices centered in children, in turn, we performed the mean of the items 3, 4, 6, 9, 15 and 17.
18 Higher mean values indicated higher use of the respective practice.
The screen time experienced by nurslings during meals was assessed with the following specific question conceived for the study: "the child watches electronic media during meals?", which could be answered with "yes" or "no".
The database was built with the Statistical Package for the Social Sciences (SPSS) software, version 22.0, with double typing and posterior validation.
The continuous parametric variables were described with the mean and standard deviation (± SD), whilst the non-parametric variables were presented by the median and interquartile range [P
25 – P
75]. The categorical variables received description by means of the absolute frequency (n) and relative frequency (%).
The variables were initially selected by bivariate analysis (
p<0.20), and posteriorly, included in the multiple linear regression. The final model was adjusted, maintaining only the variables with statistical significance (
p<0.05). The linear regression was used to estimate average differences and the 95% confidence intervals (95%CI), attempting to investigate the relationship between the outcome (scoring in the fussing scale) and the exposition (parenting practices). We performed multiple, crude and adjusted models of linear regression.
In order to compare scores of fussing and parenting practices between the male and female genders and between the different classifications of BMI/A, we used the t Student test. In addition, the potential association of nutritional status of the nursling with the screen time during meals was assessed with the Pearson's chi-square test. For all of these analyses, we adopted a 5% significance level (
p<0.005).
The study was approved by the Research Ethics Committee of the Teaching Hospital of Porto Alegre, under number 2019-0230 (CAAE:01537018.5.0000.5327) and registered in the Brazilian Registry of Clinical Trials (ReBEC – Portuguese acronym), under the identification RBR-229 scm.
ResultsIn total, data from 139 participants were analyzed. The characteristics of the sample were presented in Table 1. The sample was predominantly composed of white mothers (85.5%), who lived with a partner (82.7%), had higher education (71%) and were primiparas (80.6%), mean age of 33 years and median of family monthly income of R$6,000.00 [4,000 – 10,000]. Of the nurslings, 54% (n=75) were male, 69.5% (n=89) were eutrophic and 83.8% (n=114) did not have any screen time during meals.
We observed that the mean (±SD) of food fussiness in the sample, according with the CEBQ, was 2.88 (±0.34). With regard to the parenting practices, the sample scoring, according to the PFSQ, was 2.10 (±0.58) forparent-centered practices/high control, 1.44 (±0.33) for parent-centered practices/contingency managementand 3.0 8 (±0.69) forchild-centered practices.
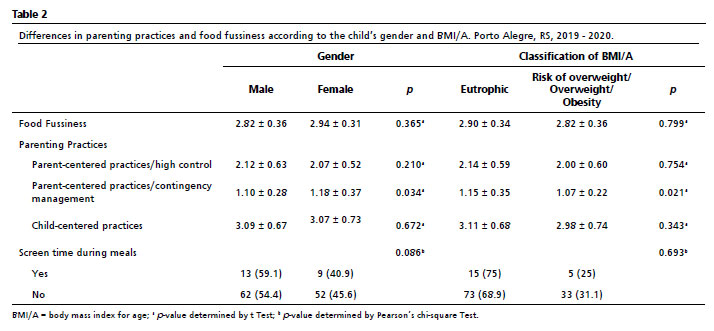
The differences in food fussiness and parenting practices according to the gender of the nursling and to the BMI/A classification are shown in Table 2. According to data shown, we could perceive that the variable that presented statistically significant difference between genders (
p=0.034) and between the different BMI/A classifications (
p=0.021) was "parent-centered practices/contingency management", whose use was higher in female nurslings and children considered eutrophic.
In turn, food fussiness, parent-centered practices/high control, child-centered practicesand screen time during meals by the nurslings did not present a statistically significant difference between genders and those with higher or lower BMI/A (
p>0.05).
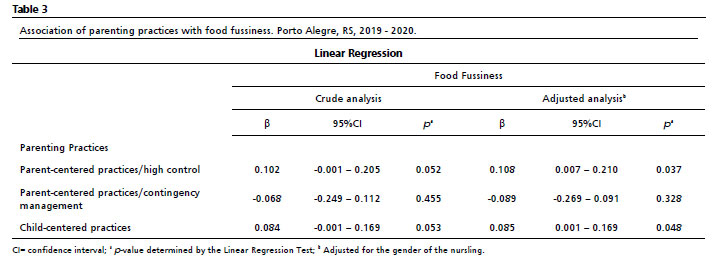
A multiple linear regression model was built in order to assess the association of food fussiness with parenting practices (Table 3). In the crude analysis, theparent-centered practices/high control, child-centered practicesand parent-centered practices/contingency managementdid not present statistically significant associations with food fussiness. When adjusting to nursling's gender, the association of parent-centered practices/high controland fussiness and child-centered practicesand fussiness became statistically significant (
p=0.037 and
p=0.048, respectively), higher in female nurslings.
Lastly, we assessed the association of nurslings' screen time during meals with food fussiness (data not available in tables). The nursling who had screen time during meals (n=22) presented a mean of food fussiness of 2.93±0.44, whilst those who did not had screen time (n=114) had a mean of food fussiness of 2.86±0.32. The difference between groups was not statistically significant (
p=0.076), according to the analysis performed with the
t test.
DiscussionIn the present study, we found an association of parenting practices with food fussiness in nurslings with 12 months of age. These findings suggest that the use of parent-centered practices/high controland the use of child-centered practicesare associated with higher food fussiness of these nurslings. In addition, the use of parent-centered practices/contingency managementis associated with lower food fussiness, however not significantly.
Additional studies that investigated parenting practices characterized by high level of control, such as the action of persuading the children to eat determined foods, also identified a positive association of this parenting behavior with the occurrence of food fussiness in childhood, suggesting that this action may intensify or perpetuate standards of selectivity, impairing a broader acceptance of foods.
9,20 This probably occurs due to the negative impact of pressure on the child's emotional status, who becomes to associate food with bad feelings, leading to lower pleasure in eating.
The results indicating that parenting child-centered practicesare associated with higher food fussiness diverge with the findings of the current literature. Previous studies demonstrated that more structured and responsive meals, that promote higher autonomy for children and that possess a positive emotional environment – characteristics ofchild-centered practices– are associated with more positive eating behaviors, more pleasure with food and less fussiness.
7,8,10,21 This divergence of results may be justified by different manners to assess parenting practices and family environment, which impairs the comparison of results of different surveys.
The findings that indicate that parent-centered practices/contingency managementcould be a protective factor for fussiness, in turn, corroborate other studies partially. This occurs due to the fact that parenting practices of management of contingencies analyzed in this survey encompasses the use of rewards and blackmail, related to food or not. With regard to the use of food rewards, previous studies found positive association of this practice with fussiness.
7,20 This suggests that food rewards encourage children to become more interested in the food offered as reward, and lower interest for the food that was intended to have its intake increased at first. On the other hand, the use of rewards that are not foods may encourage the children to try new foods, favoring the increase of foods that they like, since the taste adapts and becomes more favorable to flavor after many experiences.
20,22 The inclusion of non-food rewards in the analyses could, then, explain this potential negative association of practices of management of contingencies with food fussiness, even though the association is not significant in the statistical point of view.
Although fussiness has been associated with some practices, this fact does not mean that the practice itself is causing or preventing fussiness. The relationship between parents and children during meals is bi-directional, that is, at the same time that practices are affecting the eating behavior of children, this behavior is influencing the practices of parent as well.
23All practices studied in this study seek to expand the food intake of the child, by means of persuasion, use of rewards or the playfulness of the feeding process. Studies suggest that parents choose their feeding strategies in response to the weight of the child.
9,10 This may explain the fact that all practices were more frequent within eutrophic children, compared to those with higher BMI/A, since the concern in increasing food intake is higher for children that are thinner, highlighting the significant association only forparent-centered practices/contingency management.
We also analyzed whether there was any difference in the use of practices depending on the gender of nurslings, and found a statistically significant difference among them in the management of contingencies, with higher use in female nurslings. We did not find any data in the literature that justify such finding. However, the choice for parenting practices in response to the gender of the child may be explained by the gender expectations of the society. Nonetheless, other variables that were not analyzed may be affecting the results and further studies are necessary to investigate such association.
With regard to food fussiness, we did not find significant differences in the level of fussiness among genders, a result that corroborates the finding of previous studies.
24,25 Also, we did not observe any significant differences in the level of fussiness among BMI categories. Although some studies had associated food fussiness with a lower BMI, related to decrease of food intake common to this behavior,
26 other studies suggest that selective children frequently consume ultra-processed foods or those with high sugar levels.
2,4,21 This eating standard may contribute to avoid a significant decrease in the weight of these children, even with a lower total food intake.
A concerning data found in this survey was the high screen time experienced by nurslings during meals, which was observed in more than 15% of the sample, contradicting WHO recommendations and those from the Brazilian Society of Pediatrics.
27,28 However we did not observe association with BMI/A in this sample, it is possible that negative effects, such as irritability, sleep disorders and obesity appear in the future. We recommend substituting the screen time for interactions with caregivers in order to promote healthier habits.
Although we did not find statistically significant association of screen time with food fussiness, data suggest that children that use electronic devices during meals demonstrate higher fussiness, corroborating previous studies.
8,22 This may be explained by the lower attention to the act of eating itself, decreasing the desire for food. Moreover, screen time during meals lead the latter to cease to be moments of family interaction, which are essential to the development of healthy eating habits, and impair the observation and imitation of positive eating habits of adults.
8,22The results found cannot be generalized, due to the high socioeconomic characteristics of the sample, which are not similar to those of the general population of our country. Another limitation to be highlighted is the fact that the early enrollment and data collection were performed only with mothers, since they participated in the intervention. However, the subsequent questionnaires could be answered by any family member involved inthe child's feeding. We highlight that both parenting practices and fussiness were analyzed by the perception and report of parents, which may be passible of subjectivity and memory bias. Still, the age of assessed children is also a limitation of the study, since at 12 months of age the nursling is starting to learn about foods. The fussiness becomes more prevalent as the child is developing a higher sense of autonomy and expressing his/her preferences more firmly. In addition, it is important to highlight that due to the cross-section design of the study, it is not possible to infer a causality relationship between the studied variables.
The evidence that parenting practices in feeding are associated with food fussiness in children reinforces the importance of initiatives that focus on adequate guidance for parents in this stage of life. Even though the relationship between the two variables is bi-directional, the literature shows many of these practices are not effective to modify the children's eating behavior and that we should, accordingly, search for other strategies to solve the problem. In this way, more surveys are necessary to investigate the bi-directionality of variables and better manners to modify infant eating behavior in a positive way.
References1. Chilman L, Kennedy-Behr A, Frakking T, Swanepoel L, Verdonck M. Picky eating in children: A scoping review to examine its intrinsic and extrinsic features and how they relate to identification. Int J Environ Res Public Health. 2021 Aug; 18 (17): 9067.
2. Taylor CM, Wernimont SM, Northstone K, Emmett PM. Picky/fussy eating in children: Review of definitions, assessment, prevalence and dietary intakes. Appetite. 2015 Dec; 95: 349-59.
3. Taylor CM, Northstone K, Wernimont SM, Emmett PM. Macro- and micronutrient intakes in picky eaters: a cause for concern? Am J Clin Nutr. 2016 Dec; 104 (6): 1647-56.
4. Li P, Ren Z, Zhang J, Lan H, Man-Yau Szeto I, Wang P, Zhao A, Zhang Y. Consumption of Added Sugar among Chinese Toddlers and Its Association with Picky Eating and Daily Screen Time. Nutrients. 2022, Apr 28; 14 (9): 1840.
5. Barse LM, Tiemeier H, Leemakers ETM, Vortman T, Jaddoe VWV, Edelson LR, et al. Longitudinal association between preschool fussy eating and body composition at 6 years of age: The Generation R Study. Int J Behav Nutr Phys Act. 2015; 12 (1): 153.
6. Grulichova M, Kuruczova D, Svancara J, Pikhart H, Bienertova-Vasku J. Association of Picky Eating with Weight and Height-The European Longitudinal Study of Pregnancy and Childhood (ELSPAC-CZ). Nutrients. 2022 Jan; 14 (3): 444.
7. Finnane JM, Jansen E, Mallan KM, Daniels LA. Mealtime structure and responsive feeding practices are associated with less food fussiness and more food enjoyment in children. J Nutr Educ Behav. 2017 Jan; 49 (1): 11-8.
8. Cole NC, Musaad SM, Lee SY, Donovan SM, Strong Kids Team. Home feeding environment and picky eating behavior in preschool-aged children: A prospective analysis. Eating Behav. 2018; 30: 76-82.
9. Rendall S, Dodd H, Harvey K. Controlling feeding practices moderate the relationship between emotionality and food fussiness in young children. Appetite. 2022; 178: 106259.
10. Powell F, Farrow C, Meyer C, Haycraft E. The importance of mealtime structure for reducing child food fussiness: Mealtime structure and child food fussiness. Maternal Child Nutr. 2017 Apr; 13 (2): e12296.
11. Nunes LM, Führ J, Belin CHS, Moreira PR, Neves RO, Brito ML, et al. Correction to: Complementary feeding methods in the first year of life: a study protocol for a randomized clinical trial. Trials. 2021 Nov; 22 (1): 819.
12. World Health Organization (WHO). Anthro for personal computers, version 3.2.2, 2011: Software for assessing growth and development of the world's children. Geneva: WHO; 2010. [access in 2023 Dez 3]. Available from:
http://www.who.int/childgrowth/software/en/13. Ministério da Saúde (BR), Secretaria de Atenção à Saúde, Departamento de Atenção Básica. Orientações para a coleta e análise de dados antropométricos em serviços de saúde: Norma Técnica do Sistema de Vigilância Alimentar e Nutricional – SISVAN. Brasília (DF): Ministério da Saúde; 2011. [access in 2023 Dez 3]. Available from:
https://www.gov.br/saude/pt-br/composicao/saps/vigilancia-alimentar-e-nutricional/arquivos/orientacoes-para-a-coleta-e-analise-de-dados-antropometricos-em-servicos-de-saude14. Wardle J, Guthrie CA, Sanderson S, Rapoport L. Development of the Children's Eating Behaviour Questionnaire. J Child Psychol Psychiatry. 2001; 42 (7): 963-70.
15. Viana V, Sinde S. O comportamento alimentar em crianças: estudo de validação de um questionário numa amostra portuguesa (CEBQ). Anál Psicol. 2008; 26 (1): 111-10.
16. Komninou S, Halford JCG, Harrold JA. Differences in parental feeding styles and practices and toddler eating behaviour across complementary feeding methods: managing expectations through consideration of effect size. Appetite. 2019 Jun; 137: 198-206.
17. Purwaningrum DN, Arcot J, Hadi H, Hasnawati RA, Rahmita RS, Jayasuriya. A cultural adaptation and validation of a child eating behaviour measure in a low- and middle-income country. Public Health Nutr. 2020 Aug; 23 (11): 1931-8.
18. Cauduro GN, Reppold CT, Pacheco JTB. Adaptação Transcultural do Questionário de Estilos Parentais na Alimentação (QEPA). Aval Psicol. 2017; 16 (3): 293-300.
19. Santos KF, Coelho LV, Romano MCC. Comportamento dos pais e comportamento alimentar da criança: revisão sistemática. Rev Cuidarte. 2020; 11 (3): e1041.
20. Monnery-Patris S, Rigal N, Peteuil A, Chabanet C, Issanchou S. Development of a new questionnaire to assess the links between children's self-regulation of eating and related parental feeding practices. Appetite. 2019 Jul; 138: 174-83.
21. Vidal L, Iragola V, Machín L, Brunet G, Girona A, Cururchet MR, et al. A qualitative exploration of parents' food choices during early childhood. J Nutr Educ Behavior. 2022 Aug; 54 (8): 764-75.
22. Rahill S, Kennedy A, Kearney J. A review of the influence of tathers on children's eating behaviours and dietary intake. Appetite. 2020; 147: 104540.
23. Jansen PW, Barse LM, Jaddoe VWV, Verhulst FC, Franco OH, Tiemeier H. Bi-directional associations between child fussy eating and parents' pressure to eat: Who influences whom? Physiol Behavior. 2017; 176: 101-6.
24. Cole NC, An R, Lee SY, Donovan SM. Correlates of picky eating and food neophobia in young children: a systematic review and meta-analysis. Nutr Rev. 2017; 75 (7): 516-32.
25. Babik K, Patro-Gołąb B, Zalewski BM, Wojtyniak K, Ostaszewski P, Horvath A. Infant feeding pratices and later parent-reported feeding difficulties: a systematic review. Nutr Rev. 2021; 79 (11): 1236-58.
26. Viana V, Sinde S, Saxton JC. Children's Eating behaviour questionnaire: associations with BMI in Portuguese children. British J Nutr. 2008; 100 (2): 445-50.
27. World Health Organization (WHO). Guidelines on physical activity, sedentary behaviour and sleep for children under 5 years of age. Geneva: WHO; 2019. [access in 2023 Dez 3]. Available from:
https://www.who.int/publications/i/item/978924155053628. Sociedade Brasileira de Pediatria (SBP). Manual de Orientação #MENOS TELAS #MAIS SAÚDE. Rio de Janeiro: SBP; 2019. [access in 2023 Dez 3]. Available from:
https://www.sbp.com.br/fileadmin/user_upload/_22246c-ManOrient_-__MenosTelas__MaisSaude.pdfAuthors' contribution: Peres Loureiro G, Ficagna CR, Moreira PR: data analysis, literature review, writing and review of the manuscript. Nunes LM: professor of the research team, data analysis, review of the manuscript. Bernardi JR: coordinator of the research, data analysis, review of the manuscript. All authors approve the final version of the article and declare no conflict of interest.
Received on April 11, 2024
Final version presented on December 11, 2024
Approved on December 13, 2024
Associated Editor: Gabriela Buccini


 ; Cátia Regina Ficagna2,3
; Cátia Regina Ficagna2,3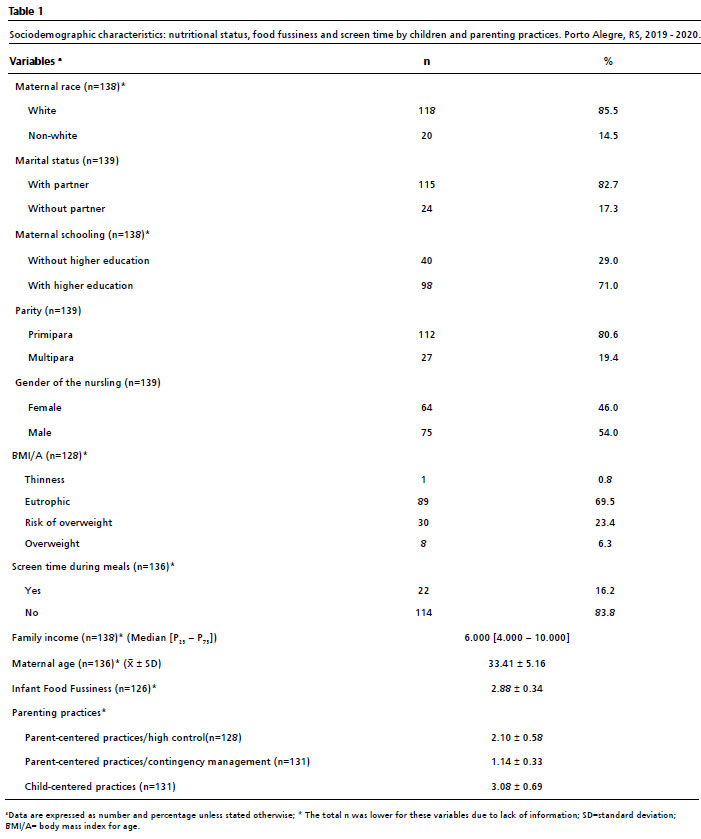






 Ler em português
Ler em português