ABSTRACT
OBJECTIVES: to analyze sexual function and predictors of sexual dysfunction among pregnant women followed up in Primary Health Care in a city in the north of Minas Gerais.
METHODS: a cross-sectional, analytical study carried out with 1,279 pregnant women in Montes Claros/MG, between 2018 and 2019. Variable: dependent sexual satisfaction; independent variables: sociodemographic and obstetric characteristics, physical and mental health conditions and complaints during pregnancy.
RESULTS: the prevalence of sexual dysfunction was 27.4%. There was an association: between nine and 11 years of schooling (PR=1.08; 95%CI=1.03-1.14; p=0.002); or more than 11 years of schooling (PR=1.14; 95%CI=1.08-1.20; p<0.001); family income ≤ 1 minimum wage (PR=1.06; 95%CI=1.02-1.09; p<0.001); gestational complaint of dizziness (PR=1.54; 95%CI=1.23-1.92; p<0.001); low social support (PR=1.53; 95%CI=1.24-1.89; p<0.001); negative body image (PR=1.26; 95%CI=1.03-1.54; p=0.020); and presence of stress symptoms (PR=1.27; 95%CI=1.00-1.60; p<0.001).
CONCLUSION: predictors of sexual dysfunction were identified in a significant proportion in pregnant women and were associated with sociodemographic factors (years of schooling); family income; obstetric factors (gestational complaints such as dizziness); social aspects such as low support; emotional aspects (negative body image) and the presence of stress symptoms. The results indicate the need for more studies on pregnant women in order to understand the causes of sexual dysfunction and provide guidance on interprofessional actions that promote sexual and reproductive health.
Keywords:
Sexuality, Pregnancy, Quality of life, Sexual behavior, Primary health care
RESUMO
OBJETIVOS: analisar a função sexual e fatores preditores de disfunção sexual entre gestantes acompanhadas na Atenção Primária à Saúde em município no norte de Minas Gerais.
MÉTODOS: estudo transversal, analítico realizado com 1.279 gestantes de Montes Claros/MG, entre 2018 e 2019. Variável: dependente satisfação sexual; variáveis independentes: características sociodemográficas, obstétricas, condições de saúde física e mental e queixas na gestação.
RESULTADOS: a prevalência de disfunção sexual foi de 27,4%. Verificou-se associação com: ter entre nove a 11 anos de estudo (RP=1,08; IC95%=1,03-1,14; p=0,002); ou mais do que 11 anos de estudo (RP=1,14; IC95%=1,08-1,20; p<0,001); renda familiar ≤1 salário mínimo (RP=1,06; IC95%=1,02-1,09; p<0,001); queixa gestacional de tontura (RP=1,54; IC95%=1,23-1,92; p<0,001); baixo apoio social (RP=1,53; IC95%=1,24-1,89; p<0,001); imagem corporal negativa (RP=1,26; IC95%=1,03-1,54; p=0,020); e presença de sintomas de estresse (RP=1,27; IC95%=1,00-1,60; p<0,001).
CONCLUSÃO: fatores preditores de disfunção sexual foram identificados em parte expressiva das gestantes sendo associados a fatores sociodemográficos (anos de estudo); renda familiar; fatores obstétricos (queixas gestacionais como a tontura); aspectos sociais como o baixo apoio; aspectos emocionais (imagem corporal negativa) e a presença de sintomas de estresse. Os resultados indicam a necessidade de mais estudos com gestantes para entender causas da disfunção sexual e orientar ações interprofissionais que promovam a saúde sexual e reprodutiva.
Palavras-chave:
Sexualidade, Gestação, Qualidade de vida, Comportamento sexual, Atenção primária à saúde
IntroductionThe construction of motherhood is one of the most important periods in women's lives. However, this period involves changes in the physical, psychological, hormonal, family, social, economic and work structures, which influence women's sexual behavior during pregnancy,
1 showing greater vulnerability to triggering or worsening sexual difficulties.
2Sexual function is an important aspect of general physical and emotional well-being, and its changes during pregnancy can have an impact on a woman's quality of life. In the literature, it has been shown that female sexual function and sexual health in pregnancy generally decrease and remain low in the postpartum period.
3In this context, women may feel insecure during sexual intercourse, fearing their partner's arousal face the changes resulting from pregnancy, and, conversely, men may not feel included in the mother-child relationship, given their partner's dedication to the pregnancy.
4 In addition, female sexual satisfaction can be influenced by multiple psychological factors; the bond between the couple, the support and involvement offered by the partner during the gestational process, myths, taboos, beliefs, religious and the couple's socio-cultural issues.
3,5,6 Other conditions, such as physical and hormonal changes resulting from pregnancy, can also interfere in a woman's pleasure, lubrication and orgasm and compromise sexual satisfaction.
6,7Although changes in sexual function during pregnancy affect women's quality of life,
7,8 this is a scarce topic in the literature, little is addressed by health professionals in their care practice and in need of further research. With this in mind, the aim of this study was to analyze sexual function and the predictors of sexual dysfunction among pregnant women followed up in Primary Health Care in a city in the north of Minas Gerais.
MethodsThis is a cross-sectional, quantitative analytical study that is part of the research entitled "
Estudo ALGE - Avaliação das condições de saúde das gestantes de Montes Claros – MG (ALGE Study - Evaluation of the health conditions of pregnant women in Montes Claros – MG) a longitudinal study", which consists of a population-based observational epidemiological survey, with a cross-sectional and analytical design, nested in the ALGE cohort.
9The city that is the setting for this study is located in the north region of the State of MG - Brazil. It is a hub in the region where it is located, whose population at the time was 417,478 inhabitants, with an average
Índice de Desenvolvimento Humano Municipal (IDH-M) (Municipal Human Development Index (MHDI) of 0.770 and a Gini Index of 0.5391.
10 The city stands out in the provision of health services, with the Family Health Strategy (FHS) that makes up the Primary Health Care (PHC), the main form of organization of local Primary Care, with 100% of the population covered with 135 family health teams at the time of the research (2018-2019). There are residency programs in Family and Community Medicine, Multiprofessional Residency in Family Health, Mental Health and Obstetric Nursing, linked to PHC and working in the FHS.
11The sample was calculated to estimate a prevalence of 50%, with a CI of 95% and precision of 2%, including correction for a finite population (N=1,661) and an additional 20% for losses, totaling 1,180 pregnant women distributed proportionally among the 15 FHS centers. All the pregnant women were initially invited and selected by simple random drawing. In total, 1,279 pregnant women took part, more than the minimum number, ensuring greater representativeness.
Thus, the sample included pregnant women who were regularly registered with the FHS and of any gestational age, while women with cognitive impairment and/or severe mental disorders, as reported by the FHS team or informed by family members, and pregnant twins, were excluded.
Data collection was carried out between October 2018 and November 2019, through interviews at the FHS health units and/or in the participants' homes, by a multi-professional team made up of professionals from the fields of nursing, medicine, nutrition and physical education, as well as undergraduate students linked to scientific initiation, and took place individually at a place and time previously defined with the pregnant woman, with an average duration of one hour each interview.
For data collection, a structured questionnaire was used with questions designed by the authors and with validated instruments, which covered sociodemographic and obstetric characteristics, physical and mental health conditions, as well as complaints during pregnancy.
In this study, the sociodemographic characteristics of the pregnant women were analyzed and a questionnaire was used for data collection which included the dependent variable: sexual satisfaction and the independent sociodemographic and economic variables age group (up to 19 years old, 20 to 35 years old, over 35 years old); marital status (living without or with a partner); schooling (primary, secondary and higher education); family income (up to two minimum wages or more than two minimum wages); occupation, social support (high social support or low social support).
Sexual satisfaction was assessed using the Sexual Quotient - Female Version (QS-F), an instrument developed by the Sexuality Studies Program (ProSex) at the
Universidade de São Paulo12 (University of São Paulo). The QS-F consists of 10 questions, organized on a Likert scale from 0 to 5, divided into five specific areas: sexual desire and interest (questions 1, 2 and 8); foreplay (question 3); personal arousal and harmony with the partner (questions 4 and 5); comfort (questions 6 and 7); and orgasm and satisfaction (questions 9 and 10). To obtain the total index, the sum of the 10 answers is multiplied by two, resulting in a value ranging from 0 to 100, where higher values indicate greater satisfaction and sexual performance.
In order to assess social support, the Medical Outcome Studies (MOS) scale was used, which contains 19 questions in which the participant indicated how often they considered each type of support: never (0), rarely (1), sometimes (2), almost always (3) and always (4). The instrument covers five dimensions of social support: material (four questions: provision of practical resources); affective (three questions: physical displays of love and affection); emotional (four questions: expressions of understanding and feelings of trust); positive social interaction (four questions: availability of people to have fun and relax with) and information (four questions: availability of people to get advice or guidance from). The closer the final score was to 100, the better the social support. The overall score of the scale was calculated from the total sum of the 19 items and the result above 66, which corresponds to the second tertile, was considered to be high social support.
13The Body Attitudes Questionnaire (BAQ), an instrument validated in Brazil by Scagliusi
et al. The instrument has 44 items on a Likert scale with five response options ("I totally agree" to "I totally disagree"). The total BAQ score is the sum of the scores for each item. This value ranges from 44 to 220 points, and the higher the score, the greater the dissatisfaction with body image on the six subscales: "physical attractiveness", "self-deprecation", "total fat", "body protrusion", "perception of lower body fat" and "strength and physical fitness".
14The obstetric characteristics investigated were the gestational trimester (1
st, 2
nd and 3
rd), the planning of the current pregnancy (yes or no) and parity (nulliparous, primiparous or multiparous). The following self-reported health conditions were investigated: urinary infection, gestational diabetes, anemia, hemorrhage, hypertensive syndromes in pregnancy (HSP) and migraine. The presence of the main complaints during pregnancy was also investigated: sleep-related; cardiovascular (edema, epistaxis, hemorrhoids, palpitation, bleeding gums, varicose veins); skin (chloasma, stretch marks); gastrointestinal (constipation, abdominal pain, eructation, nausea, heartburn, vomiting, salivation); breast (mastalgia); musculoskeletal (cramps, low back pain); neurological (headache, paresthesia); respiratory (shortness of breath, nasal obstruction); weakness, dizziness and fainting. These conditions and complaints were addressed because they are among the main risk conditions in pregnancy, based on recommendations from the Brazilian Ministry of Health for low-risk prenatal care in PHC.
15The mental health conditions examined were anxiety symptoms (low or high level) and stress levels (low and high level). To analyze the level of anxiety, the short version of the Brazilian
Inventário de Anxiedade Traço-Estado (IDATE) (State-Trait Anxiety Inventory) was used in its validated version in Brazilian Portuguese.
16 The IDATE provides a reliable measure for two components of anxiety: state and trait. On the IDATE, the person describes how they feel "now, at this moment" in relation to six items presented on a four-point Likert scale: 1 (absolutely not); 2 (a little); 3 (quite a lot); 4 (very much). In the trait-IDATE, the participant answers how they "usually feel" for the remaining six items, which are arranged according to a new four-point Likert scale: 1 (almost never); 2 (sometimes); 3 (often); 4 (almost always). The scores for the positive questions are reversed, i.e. 1, 3 and 5 on the state-IDATE and 1, 3 and 6 on the trait-IDATE. The scores are obtained by adding up the answers, with 6 being the minimum score and 24 the maximum, for both state and trait. As there is no cut-off point for the reduced form, and because the mean and median values of the trait-IDATE in this study are close, this variable was dichotomized by the median because it is an integer. Pregnant women with a value below this were classified as having a "low level of anxiety" and those with a value above this were classified as having a "high level of anxiety".
16The level of stress was assessed using the Perceived Stress Scale (PSS-14),
17 translated and validated for the Brazilian population, which identifies situations in the individual's life that are considered stressful, establishing levels of intensity. This scale is made up of 14 items which assess the frequency with which certain feelings and thoughts have occurred in the last month, with answers ranging from zero (never) to four (always). The PSS-14 scale score is obtained by reversing the scores of the positive items and adding up the answers to the 14 items, with the total score ranging from zero (no stress symptoms) to 56 (extreme stress symptoms). In order to classify pregnant women in terms of their perceived level of stress, the scores on the PSS-14 scale were dichotomized into <28 and ≥28, with the cut-off point defined by the 75
th percentile. Pregnant women with scores <28 were classified as having a low level of stress and those with scores ≥28 as having a high level of stress.
17The statistical program SPSS version 22.0 (SPSS
® IBM
® Inc., Chicago, USA) was used. The absolute and relative values of the categorical variables were calculated. Pearson's chi-squared test was used to analyze the association between the dependent variable and the other variables, followed by calculation of the prevalence ratio and its respective 95% confidence intervals. Poisson regression with robust variance was performed, selecting the variables that showed a significance level of up to 20% in the bivariate analysis. In the final model, those with a significance level of 5% remained.
The study was approved by the Ethics Committee of the
Universidade Estadual de Montes Claros (State University of Montes Claros) with Consubstantiated Opinion No. 2.483.623/2018, CAAE 80957817.5.0000.5146.
ResultsA total of 1,279 pregnant women attending PHC took part in the study. The majority were over 30 years old (51.3%), had between nine and 11 years of schooling (64.9%) and lived with a partner (72.3%). In addition, more than half had a gross family income of more than one minimum wage (76.7%) and did not work outside the home (56.4%).
As shown in Table 1, 27.4% of the pregnant women reported having sexual dysfunction. Analyzing each domain individually, we found that most of them said they had sexual desire and interest (96.9%), increased satisfaction with foreplay (96.1%), personal arousal and synchrony with their partner (96.4%). In addition, a total of 96% of pregnant women reported feeling comfortable, orgasmic and satisfied.
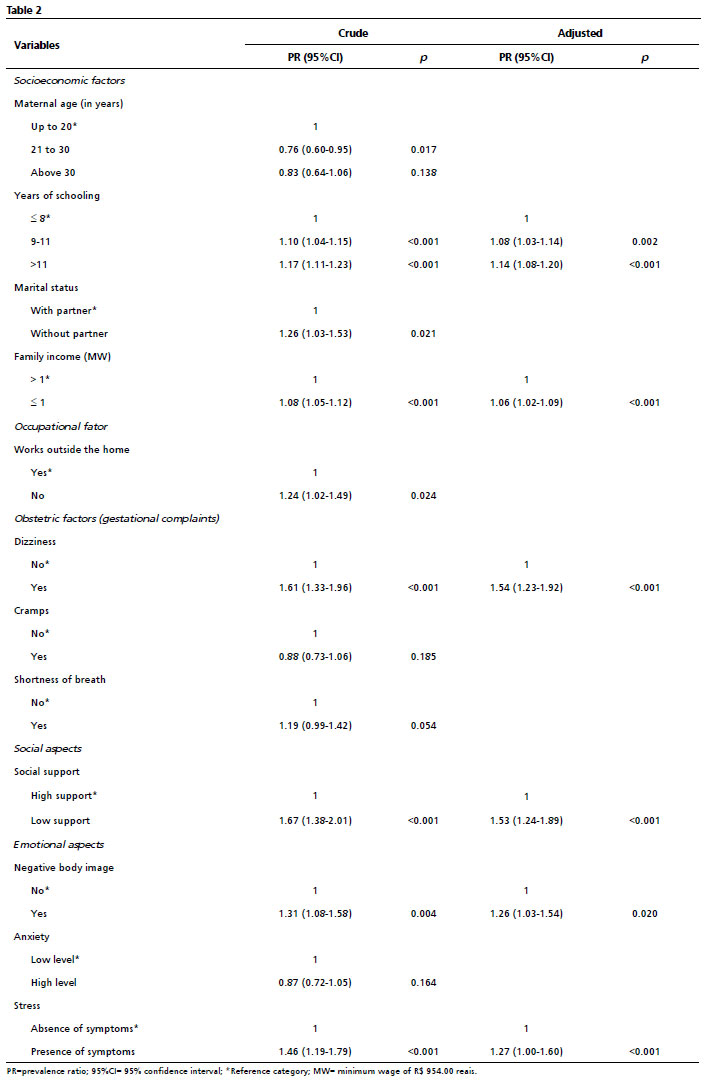
Table 2 shows the factors associated with sexual dysfunction in the pregnant women evaluated. The first association model showed that almost all the factors analyzed had significant descriptive levels (
p<0.001) in relation to the outcome variable. After adjusting the model, socioeconomic, obstetric, social and emotional factors were identified as having a significant influence on the prevalence of sexual dysfunction. The associated factors include having between nine and 11 years of schooling (PR=1.08; 95%CI=1.03-1.14;
p=0.002) or more than 11 years of schooling (PR=1.14; 95%CI=1.08-1.20;
p<0.001); family income ≤1 minimum wage (PR=1.06; 95%CI=1.02-1.09;
p<0.001); gestational complaint of dizziness (PR=1.54; 95%CI=1.23-1.92;
p<0.001); low social support (PR=1.53; 95%CI=1.24-1.89;
p<0.001); negative body image (PR=1.26; 95%CI=1.03-1.54;
p=0.020); presence of stress symptoms (PR=1.27; 95%CI=1.00-1.60;
p<0.001).
DiscussionThis study showed that more than a quarter of the pregnant women analyzed had a high prevalence of sexual dysfunction, an outcome that was associated with sociodemographic factors (years of schooling); family income; obstetric factors (gestational complaints such as dizziness); social aspects such as low support; emotional aspects (negative body image) and the presence of stress symptoms.
In the national context, a study carried out in Aracaju-SE, at the Women's Reference Center and at a Basic Health Unit, found a prevalence of sexual dysfunction in 31.7% of the monitored pregnant women.
6 Another three international studies, carried out with pregnant women in Iran, Arizona and Lebanon, although they used other assessment instruments, are consistent with the investigations that aimed to assess the sexual satisfaction of pregnant women and the factors involved that could affect sexuality during pregnancy.
18,19,20 It must be considered that the different prevalence rates of sexual dysfunction in populations can be attributed to differences in the methodological process used to investigate this condition, as well as the particularities of ethnicities, demographics and socioeconomic and cultural aspects.
When analyzing the domains that make up sexual satisfaction investigated in this study, similarities were found between the domains with the highest percentages of dissatisfaction and the domain with the lowest percentage of sexual satisfaction. Studies carried out on pregnant women in Ceará and Recife have also shown changes in the pregnant women's sexual function, with a reduction in most of the domains of sexual satisfaction.
2,4 As for the domains most affected, different results were found in a study with 358 participants, both pregnant and non-pregnant.
21In this study, desire and arousal were the most affected domains of sexual function. Together, these results show that the domains of sexual function can be influenced by different aspects in women's lives.
21 In relation to the "Foreplay" domain, a study corroborates the results presented and points to the reduction in foreplay in sexual activities during pregnancy. It is understood that sexuality is a complex process that is shaped by the culture to which the individual belongs and the social conditions in which he/she lives.
22 In this sense, sex education should be carried out by trained professionals in individual approaches or with the couple in order to help and promote adaptive behaviors during pregnancy.
2Regarding the "orgasm and satisfaction" domain, it can be considered that they are facilitated by the inclusion of sexual desire, sexual self-esteem, open communication about sexual life with the partner, the ability to concentrate during sex, the mutual initiative to relate sexually and the sexual skills of the partner.
23 The findings of this study are similar to the results of another study which showed a predominant decrease in sexual domains (desire, arousal, orgasm) and psychophysical correlates (lubrication and sexual satisfaction).
2In addition to the domains, sociodemographic factors were associated with sexual dysfunction in pregnant women. More than eight years of schooling proved to be a protective factor for this outcome. Studies corroborate that women with a higher level of education tend to have more knowledge about sexual health, as well as a greater ability to communicate with health professionals and their partners.
3,18 Higher levels of education are also associated with a more positive attitude towards sexuality and overcoming myths and taboos, making it easier to adapt to physiological changes during pregnancy.
8 Therefore, it is possible to suggest that women with more schooling have a better understanding of bodily changes and how these can impact sexuality, reducing the risk of sexual dysfunction.
18The highest prevalence of sexual dysfunction was found among pregnant women with a family income of up to one minimum wage. A study
4 highlights that socioeconomic factors are fundamental to sexual health during pregnancy and that low-income women often face difficulties in accessing adequate health services, which includes emotional support and satisfactory guidance on sexuality during prenatal care, increasing the risk of sexual dysfunction. In addition, stress related to the financial situation and the lack of adequate support can interfere with a woman's ability to fully engage in sexual relations.
Another factor associated with sexual dysfunction in pregnant women was low social support. This finding is consistent with the results of other studies which found that pregnant women with less social support had a higher prevalence of sexual dysfunction, especially in terms of reduced desire and difficulty reaching orgasm.
24,25 Social support is a critical determinant of sexual health during pregnancy
4 and the lack of adequate social support can aggravate stress, increasing the negative impacts on sexual function.
26When evaluating obstetric factors, there was a higher prevalence of sexual dysfunction among pregnant women with gestational complaints of dizziness. Different gestational complaints associated with sexual dysfunction have been found in the literature and studies have identified that symptoms such as fatigue, malaise and increased body volume were associated with a reduction in sexual satisfaction and desire.
25,26These symptoms can impair well-being in general, directly affecting pregnant women's physical and mental readiness for sexual involvement. Gestational complaints can reduce energy for physical activities, including sexuality, and can be associated with other clinical conditions, which compromise a woman's physical and emotional well-being, as well as increasing a sense of vulnerability and body insecurity, which interferes with the ability to relax and enjoy sexual relations.
23 Sexual dysfunction has also been associated with the presence of negative body image. In agreement, a cross-sectional, analytical study carried out with pregnant women in the maternity service in Tacna, Peru, pointed out that women who experienced body changes during pregnancy and had a negative perception of their body shapes reported a higher incidence of sexual dysfunction, especially in terms of decreased sexual desire and satisfaction.
24,25,26 A study investigating the body image and sexual function of Turkish pregnant women and their partners found that women's perception of their body image differed by trimester, becoming more negative in the third trimester, the same period that sexual dysfunction increased among women and their partners.
27In the scientific scenario, it is clear that negative body image directly affects women's self-esteem and emotional well-being, which impacts sexual function. Women who have negative perceptions of their body changes during pregnancy may feel less attractive and more uncomfortable with their own bodies, which leads to feelings of avoiding physical contact and less involvement in sexual relations.
26,27International literature also points to the presence of stress symptoms associated with sexual dysfunction in pregnant women, with this condition being more evident in the third trimester.
26,27 An analytical cross-sectional study of 346 women attending a maternity hospital in Tacna, Peru, found that women who experienced high levels of anxiety and stress during pregnancy reported a higher incidence of sexual dysfunction, and emphasized that stress directly affects sexual function by altering libido and reducing sexual pleasure.
25The association between stress and sexual dysfunction occurs because stress raises levels of cortisol, a hormone that, if chronically elevated, can interfere with sexual response by causing fatigue, decreased desire and difficulties with arousal and orgasm.
28 In addition, stress can aggravate concerns about pregnancy and the body, contributing to a negative body image and a cycle of anxiety, further impairing sexual function.
This study showed that the prevalence of sexual dysfunction among pregnant women is a relevant factor to evaluate, considering the various impacts this condition can have on women's quality of life and sexual function during pregnancy. This factor can be associated with multiple aspects of physical and mental health, damaging not only emotional well-being, but also a woman's interpersonal relationships. In addition, during pregnancy, hormonal and bodily changes are intense, which can aggravate problems of self-esteem and body perception, contributing to a worsening of sexual function.
25,27Despite this, the quality of sexuality during pregnancy is often neglected, and there is an urgent need for interventions.
24 Research underlines the importance of education and counseling on sexuality in prenatal care. Pregnant women who participated in educational programs on sexuality had a better understanding and management of their sexual experiences during pregnancy, resulting in greater sexual satisfaction.
2,29,30 In addition, carrying out actions to promote the health of pregnant women, with an emphasis on prenatal care, is crucial for the general well-being of these women.
In the context of the FHS, it is essential that professionals are aware of these aspects and offer a safe space for discussions about sexuality. A multidisciplinary approach and emotional support can help mitigate the effects of sexual dysfunction, providing a healthier and more harmonious pregnancy.
30 Studies indicate that adequate support and specialized counseling during prenatal care play a fundamental role in promoting sexual health.
25,26Taken together, the findings of this study provide an opportunity to discuss a subject that is still very scarce on the national scene. Furthermore, this is a population-based study with a large number of participants, which reinforced the associations identified.
This present study has limitations in terms of recall bias, as the questionnaires were administered during pregnancy, which may have altered some women's reports, as they could not remember all the reasons for not exercising sexuality, along with cultural and behavioral issues, both physical and emotional, typical of pregnancy. Another bias was the fact that only
Sistema Único de Saúde (SUS) (Public Health System) users took part, therefore belonging to a specific demographic group. We should also consider the use of self-reporting, which may be influenced by memory bias. To minimize this, validated instruments were used.
The conclusion is that sexual dysfunction was identified in a significant proportion of pregnant women monitored by the FHS teams in the city of Montes Claros. The results suggest that this outcome may be associated with sociodemographic factors, related to years of schooling and family income, obstetric aspects, evidenced by the gestational complaint of dizziness, social aspects, such as lack of social support and emotional aspects linked to body image, anxiety and stress. Understanding these problems can help health professionals plan health practices or interventions to deal with them and, in doing so, positively impact the sexual health of pregnant women.
References1. Van den Bergh BRH, van den Heuvel MI, Lahti M, Braeken M, de Rooij SR, Entringer S,
et al. Prenatal developmental origins of behavior and mental health: The influence of maternal stress in pregnancy. Neurosci Biobehav Rev. 2020; 117 (1): 26-64.
2. Pereira EV, Belém JM, Alves MJH, Torquato JA, Firmino PR, Fialho AV,
et al. Factors associated with sexual practices and positions performed by pregnant women: a cross-sectional study. Rev Bras Enferm. 2022; 75 (3): e20210162.
3. Bilgiç FŞ, Karaahmet AY. Attitudes and beliefs regarding sexuality in pregnancy affect sexuality Turkey example: A cross-sectional study. Eur J Obstet Gynecol Reprod Biol. 2022; 276: 14-20.
4. Guendler JA, Katz L, Flamini MEDM, Lemos A, Amorim MM. Prevalence of Sexual Dysfunctions and their Associated Factors in Pregnant Women in an Outpatient Prenatal Care Clinic. Rev Bras Ginecol Obst. 2019; 41: 555-63.
5. Rocha FDA, Fensterseifer L. A função do relacionamento sexual para casais em diferentes etapas do ciclo de vida familiar. Contextos Clín. 2019; 12 (2): 1-24.
6. Soares PRAL, Calou CGP, Ribeiro SG, Aquino PS, Almeida PC, Pinheiro AKB. Sexualidade em gestantes e fatores de risco associados. Rev Bras Enferm. 2020; 73 (Supl. 4): e20180786.
7. Fernández-Sola C, Huancara-Kana D, Granero-Molina J, Carmona-Samper E, López-Rodríguez MM del, Hernández-Padilla JM. Sexualidade durante todas as fases da gravidez: experiências de gestantes. Acta Paul Enferm. 2018; 31 (3): 305-12.
8. Rivemales MC, Lacava RM. Cuidando do prazer no pré-natal: disfunção sexual na gravidez. Rev Baiana Saúde Pública. 2021;43(4): 135-45.
9. Merchán-Hamann E, Tauil PL. Proposal for classifying the different types of descriptive epidemiological studies. Epidemiol Serv Saúde. 2021; 30 (1): e2018126.
10. Instituto Brasileiro de Geografia e Estatística (IBGE). Censo Demográfico, 2019. [access in 2024 Nov 30]. Available from:
https://cidades.ibge.gov.br/brasil/mg/montes-claros/panorama11. Ministério da Saúde (BR). Cobertura da Atenção Básica (2007-2020): cobertura populacional estimada de equipes de saúde da família (eSF) e de equipes de Atenção Básica (eAB). [
Internet]. [access in 2024 Nov 30]. Available from:
https://relatorioaps.saude.gov.br/cobertura/ab12. Abdo AHN. Quociente sexual feminino: um questionário brasileiro para avaliar a atividade sexual da mulher. Diagn Tratamento. 2009;14 (2): 89-1.
13. Griep RH, Chor D, Faerstein E, Werneck GL, Lopes CS. Validade de constructo de escala de apoio social do Medical Outcomes Study adaptada para o português no Estudo Pró-Saúde. Cad Saúde Pública. 2005; 21 (3): 703-14.
14. Meireles JFF, Neves CM, Carvalho PHB, Ferreira ME. Imagem corporal, atitudes alimentares, sintomas depressivos, autoestima e ansiedade em gestantes de Juiz de Fora, Minas Gerais, Brasil. Ciênc Saúde Colet. 2017; 22 (2): 437-45.
15. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Atenção ao pré-natal de baixo risco. Brasília (DF): Ministério da Saúde; 2012. [access in 2024 Out 6]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/cadernos_atencao_basica_32_prenatal.pdf16. Fioravanti-Bastos ACM, Cheniaux E, Landeira-Fernandez J. Development and validation of a short-form version of the Brazilian state-trait anxiety inventory. Psicol Reflex Crít. 2011; 24 (3): 485-94.
17. Luft CDB, Sanches SO, Mazo GZ, Andrade A. Versão brasileira da Escala de Estresse Percebido: tradução e validação para idosos. Rev Saúde Pública. 2007; 41 (4): 606-15.
18. Alidost F, Dm SJ, Nasiri M, Reisabdollahi H, Pakzad M, Hadi M,
et al. The Relationship Between the Wealth Index and Pregnancy-Related Anxiety in Each Trimester of Pregnancy and Their Effect on Sexual Dysfunction. Bangladesh J Med Sci. 2021; 20 (2): 401-8.
19. Gerges S, Obeid S, Hallit S. Associations Between Eating Attitudes, Mental Health, and Sexual Dysfunction during Pregnancy. J Sex Marital Ther. 2022; 25: 517-32.
20. Angin AD, Ozkaya E, Cetin M, Gun I, Sakin O, Ertekin LT,
et al. Comparison of Female Sexual Function and Sexual Function of Their Partners Between Groups of Pregnant and Non-Pregnant Women. Ginekol Pol. 2020; 91 (5): 235-9.
21. Gonçalves GB, Rodrigues E, Moura Siqueira GF, Filho RPPA,
et al. A sexualidade na gestação e seus impactos na qualidade de vida das gestantes: uma revisão. Braz J Health Rev. 2022; 5 (4): 16696-706.
22. Şolt Kırca A, Dagli E. Sexual attitudes and sexual functions during pregnancy: A comparative study. Eur J Obstet Gynecol Reprod Biol X. 2023 Jul 7; 19: 100215.
23. Kontula O, Miettinen A. Determinants of female sexual orgasms. Socioaffective Neurosci Psychol. 2016; 6 (4):1-22.
24. García DS, Soriano N, FischerSuárez N, Castro Luna G, Parron Carreño T, Aguilera Manrique G. Quality of Sexuality during Pregnancy, We Must Do Something—Survey Study. Int J Environ Res Public Health. 2023; 20: 965.
25. Sologuren-García G, Linares CL, Flores JR, Mejia CR. Ejercicio de la sexualidad en gestantes de Tacna. Rev Chil Obstet Ginecol. 2020; 85 (6): 584-94.
26. Olivares-Noguera E, Montoya-Moreno RA, Arteaga-Noriega A. Prevalencia de disfunción sexual en gestantes en control prenatal en una institución hospitalaria en Rionegro, Colombia, 2020-2021. Rev Colombiana Obstet Ginecol. 2021; 72 (4): 368-376.
27. Gamusay M, Erbil N, Demirbag BC. Investigation of Sexual Function and Body Image of Pregnant Women and Sexual Function of Their Partners. Sex Relatsh Ther. 2021; 36 (3): 1-15.
28. Wright JJ, O'Connor KM. Female sexual dysfunction. Med Clin North Am. 2015; 99 (3): 607-28.
29. Everett BG, Higgins JA, Haider S, Carpenter E. Do Sexual Minorities Receive Appropriate Sexual and Reproductive Health Care and Counseling? J Womens Health. 2019; 28 (1): 53-62.
30. Mahnaz E, Nasim B, Sonia O. Effect of a structured educational package on women's sexual function during pregnancy. Int J Gynecol Obst. 2019; 148 (2): 225-30.
Authors' contribution: Oliva ALC: article design, data storage and collection, participation in data analysis and interpretation, writing of the manuscript, revision, discussion of results, revision of the manuscript.
Bacelar Tibães HB: design of the article, storage and collection of data, participation in data analysis and interpretation, writing of the manuscript, revision, discussion of the results, revision of the manuscript. Supervision of all activities.
Taffarel GG, Souza Filho JWF, Silva BRG: design of the article, storage and collection of data, participation in the analysis and interpretation of data, writing of the manuscript, revision, discussion of results.
Brito MFSF: design of the article, storage and collection of data, participation in the analysis and interpretation of data, writing of the manuscript, revision, discussion of the results, revision of the manuscript. Project supervision and administration.
Rodrigues CAO: storage and collection of data, analysis and interpretation of data, revision, discussion of the results and revision of the manuscript.
All the authors have approved the final version of the article and declare no conflict of interest.
Received on November 25, 2024
Final version presented on April 14, 2025
Approved on April 23, 2025
Associated Editor: Ricardo Cobucci


 ; Hanna Beatriz Bacelar Tibães2
; Hanna Beatriz Bacelar Tibães2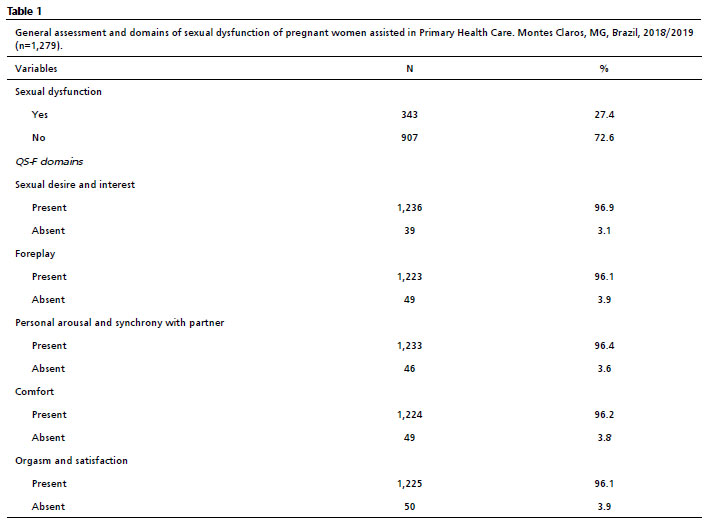






 Ler em português
Ler em português