ABSTRACT
OBJECTIVES: to develop and conduct a pilot test of a risk detection instrument for sexual domestic violence among schoolchildren aged 9 to 11 years, entitled the Risk Detection Instrument - Sexual Domestic Violence (IDR-VSD).
METHODS: this is a mixed method study conducted between January 2019 and December 2022, following the Consensus-based Standards for the Selection of Health Measurement Instruments (COSMIN) guidelines. The qualitative phase included a consensus technique with nine interprofessional experts and cognitive interviews with the target population, including schoolchildren with impairment. A pilot test was conducted with 109 participants, and internal consistency, reliability, and factor structure were analyzed.
RESULTS: the initial version comprised 22 items with playful elements, distributed across four dimensions (biological, psycho-relational, social, and ecological). The intraclass correlation coefficient was 0.602 (95%CI=0.48-0.70; p<0.001). The overall Cronbach's alpha was 0.602. After correcting the item-total correlations, the overall alpha increased to 0.654 for 18 items. One item with a measure of sampling adequacy below 0.50 was removed. Exploratory factor analysis was performed with 17 items, distributed across five factors that explained 53.76% of the total cumulative variance, in accordance with the theoretical model.
CONCLUSION: the IDR-VSD demonstrates favorable measures of reliability and factor structure, despite the complexity of the studied phenomenon.
Keywords:
Domestic violence, Sexual violence, Instrument development, Risk assessment, Child
IntroductionValidating and using instruments developed for children can contribute to identify risk contexts or early detection of violence.
1 It is estimated that approximately 20% of the women and 5–10% of the men have had experienced sexual violence during childhood, highlighting its high prevalence worldwide.
2 Child sexual abuse (CSA) related to sexual domestic violence (SDV) was chosen as the focus of this study because it represents an adverse childhood experience (ACE) with robust scientific evidence of biopsychosocial and ecological repercussions, including effects that may be transmitted throughout generations. CSA encompasses both contact and noncontact forms of sexual abuse.
2,3Nevertheless, SDV is one of the most difficult forms of violence to disclose and report, as it primarily occurs in domestic settings, often sustained by implicit codes of silence, with only the most severe cases reaching police or health emergency services.
3 There are also the prospects of co-occurrence of sexual violence (SV) with other types of violence and the poly-victimization of victimized subjects throughout their lives, further increase of biopsychosocial, ecological, and inter-generational implications for those involved. Women who experienced sexual abuse before the age of 13 had a higher risk of subsequent exposure, particularly to intimate partner violence.
4There is significant literature published on screening tools for adults and adolescents regarding situations of CSA and other types of violence that occurred at childhood.
5 However, screening for risks at childhood through self-report instruments may allow protective systems to be activated earlier, enhancing actions against health effects and costs.
6The innovation of this study lies in identifying risk factors for sexual domestic violence to enable early detection, addressing the lack of age-specific, self-report instruments focused on secondary prevention, defined as prevention targeted at risk groups.
1 The proposed instrument will be free of charge, suitable for a large-scale application, and designed to be used by a wide range of professionals (pediatricians, nurses, social workers, psychologists, teachers, etc.). As it was developed using a community-based approach within the school setting, it is intended to be applicable through diverse contexts, including schools, clinical environments, and other child-focused care settings.
Following further refinement in subsequent studies, the instrument is expected to be integrated into intersectoral child protection policies, supporting the timely identification and notification of detected risk cases by professionals to the child protection network. Most importantly, the instrument is not intended to replace the official individual violence notification forms for this age group, but rather to complement existing surveillance and report mechanisms by facilitating early risk detection and referral.
Therefore, this study aimed to develop an instrument to detect risk for SDV, using specific age to increase accuracy in risk detection. The age range chosen was in line with the determination of the limits of childhood proposed by the
Estatuto da Criança e do Adolescente7 (Brazilian Child and Adolescent Statute), corresponding to the final years of childhood (from nine to 11 years), before the onset of adolescence (at 12 years). The choice of this age group aimed to meet two conditions: the potentiality of the critical capacity of schoolchildren for the instrument in the cognitive interview
8 and the epidemiological representativeness of girls and boys in relation to report cases of SDV at childhood.
9 Our primary objective was to develop a risk detection instrument for SDV in schoolchildren from 9 to 11 years of age, called the
Instrumento de Detecção de Risco – Violência Sexual Doméstica (IDR-VSD) (Risk Detection Instrument - Sexual Domestic Violence).
MethodsThis study was approved by the Research Ethics Committee of the
Universidade Federal de Pernambuco (CAAE: 99193718.0.0000.5208). Written informed consent was obtained from parents or legal guardians, and assent was obtained from the children prior to participation. Data collection and study procedures were conducted between January 2019 and December 2022. No external funding was received for this study, and the artificial intelligence was used solely for english language editing in this study.
This work is a methodological development research. It was a mixed method study, beginning with a qualitative phase followed by the quantitative phase.
10 Publications of the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) guided the methodological path.
11 Tool development steps were carried out: narrative review with systematic search to develop a theoretical model and a matrix of descriptors for consensus technique; qualitative study with the target population; analysis of reliability (internal consistency and reproducibility), factor structure and multidimensionality of the generated instrument.
A systematic database search was conducted for the narrative review. After applying the eligibility criteria, 38 articles were selected. Books
12,13 and a Master’s thesis
14 were also consulted for the development of the theoretical model and descriptors matrix. The selection of the two theoretical frameworks was informed by prior narrative reviews and supported by the most recent systematized narrative review. Accordingly, the model was grounded in: (1) Attachment Theory,
13,15 due to its strong empirical support in studies addressing the intergenerational transmission of insecure attachment in the context of sexual domestic violence (SDV); and (2) Unified Developmental Theory,
16 for its integrative approach on biopsychological, social, ecological, and intergenerational subsystems in human development. Both theoretical frameworks are consistent with and reinforce the World Health Organization’s Ecological Model of Violence, by situating individual risk within interconnected relational, community, and societal levels.
2The Jones and Hunter Nominal Group Technique (NGT)
17 was used to qualitatively assess the relevance and comprehensiveness of the theoretical model and to develop the descriptors matrix. In June 2019, nine experts served as judges in the NGT based on their academic, professional, and scientific expertise related to the theme and object of the study. The panel included two pediatricians, three psychologists, an occupational therapist, a nurse, a public health physician, and a teacher working with socially vulnerable children. The first version of the IDR-VSD was developed by the first author (KDXB) using Microsoft Word for Windows, version 16.0. Following expert review, the instrument was approved for qualitative testing with the target population.
The cognitive interview technique proposed by Willis
18 was applied to the target population to identify potential problems in the first version of the questionnaire. Comprehensibility of instructions, items and response options were intensively discussed with the children, as well as aspects of relevance and comprehensiveness. Students of both sexes, aged 9 to 11 years, of fourth and fifth grades of the municipal public school system in Recife, Pernambuco, Brazil, participated in the study. Data collection was conducted during the first two weeks of March 2020 and involved 14 students. The COVID-19 pandemic limited the inclusion of a larger sample of students due to schools closures. The sessions with the children were conducted by the first author (KDXB) together with the research co-supervisor (UBL), a psychologist. The detailed qualitative analysis of this phase will be reported in a separate manuscript.
The pilot testing for the IDR-VSD was conducted between August 2021 and July 2022 in five additional schools within the municipal public education system, using a convenience sample. Inclusion criteria comprised students of both sexes aged 9 to 11 years, including children with impairment (hearing, visual, physical, or cognitive). The exclusion criterion was the inability to respond to the items in any format, even with support. The effects of the COVID-19 pandemic limited the number of children available to participate in the selected schools. To minimize bias, the research team did not have access to the children’s responses during the testing phase, as all questionnaires were entered using a double-entry procedure only after completion of the retest. The administration of all questionnaires was carried out exclusively by the first author (KDXB).
Throughout the research process, the study team ensured emotional care and safeguarding measures for the participating children, in collaboration with school administrators, teachers, school psychologists, and the psychologist integrated into the research team, to address and manage any potential emotional distress arising from participation. When necessary, referrals to the local healthcare network were facilitated to ensure appropriate follow-up and support for children experiencing emotional distress or identified risks.
Cognitive interviews were analyzed using a semi-structured interview guide, field notes, video recordings, and interview transcriptions. An exhaustive review of the material, based on direct observation and suggestions provided by the schoolchildren, resulted in immediate revision to the first version of the questionnaire. Based on these modifications, the second version of the IDR-VSD was developed by the authors using Microsoft Word for Windows, version 16.0.
Data analysis of the pilot test was conducted using SPSS version 22.0. The selection of statistical tests followed the methodological recommendations proposed by Hair
et al.
19 The Kolmogorov–Smirnov test (KST) was applied, along with frequent distributions and measures of central tendency and dispersion, adopting a 5% significance level. Reliability analysis comprised estimation of internal consistency using Cronbach’s alpha and evaluation of test–retest reliability using the two-way random effects intraclass correlation coefficient (ICC) for a single rater, based on absolute agreement. Exploratory factor analysis (EFA) included Bartlett’s test of sphericity (BTS), the Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy, and examination of communalities (h²) using the principal component extraction method, as well as item-level measures of sampling adequacy (MSA). The number of factors to be retained was determined based on the
eigenvalue criterion (Kaiser criterion), the slope diagram criterion (Scree test), and the percentage of variance explained. Factor rotation was performed using the oblique Promax method with Kaiser normalization, given the expected correlations among the items. The solution was iteratively refined until an optimal and interpretable factor structure was achieved.
19A systematic review was conducted to identify instruments addressing similar constructs and to select a comparator for the subsequent criterion validation stage. The review followed the updated COSMIN methodology for systematic reviews of patient reported outcome measures (PROMs). The first author was invited to participate and took part in the PRISMA-COSMIN guideline pilot test, incorporating the revisions recommended during the peer-review process into the systematic review manuscript. The review protocol was registered in PROSPERO in 2021 (registration number: CRD42021278465), and the study has been published since.
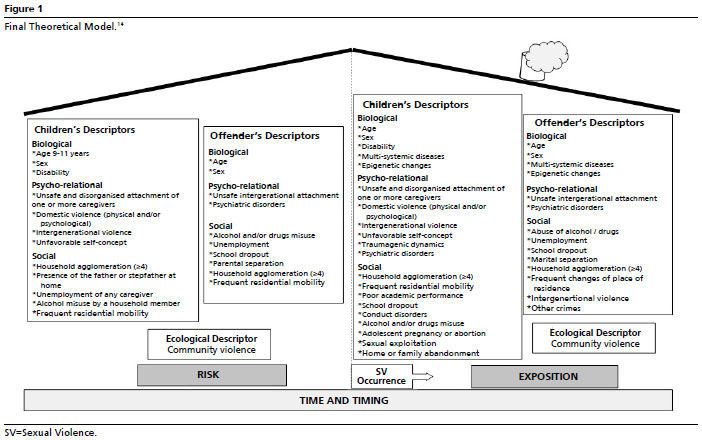
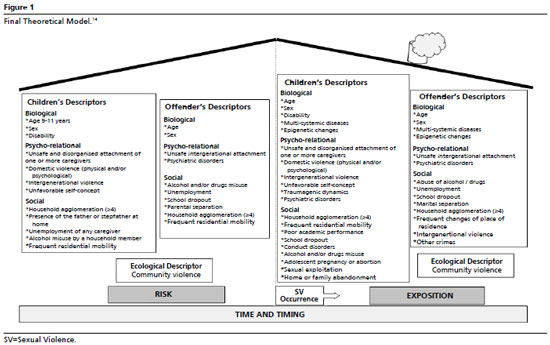
20ResultsThe construct measured by the IDR-VSD is the “risk of sexual domestic violence among schoolchildren aged 9 to 11 years”. Based on the literature review, the theoretical model was defined as multidimensional, incorporating risk factors from the perspectives of the child, the perpetrator, and their interaction. The original matrix was structured by biological, psychological, social, and ecological dimensions, considered within a spatiotemporal framework.
The face-to-face NGT meeting lasted four hours, and the group agreed that an additional meeting was not necessary. Figure 1 presents the final theoretical model resulting from the group discussions. Consensus was reached on retaining the proposed descriptors; however, two major modifications were recommended: (1) information regarding the disability descriptor should be obtained from the teacher prior to the child’s completion of the questionnaire; and (2) the psychological dimension should be expanded to include the construct of self-concept, allowing a more in-depth assessment of the psycho-relational structure. This construct was considered the most appropriate to capture the link between disorganized insecure attachment and its implications for self-perception among schoolchildren at risk of sexual domestic violence.
Accordingly, the former “Psychic Dimension” was renamed the “Psycho-relational Dimension,” with the inclusion of the descriptor “Unfavorable Self-Concept.” This construct was informed by Assis and Avanci
21 work and by the conceptual definitions underlying the Self-Concept Factor Scale.
22The final matrix also incorporated the following substructures within the construct “Disorganized Insecure Attachment of One or More Caregivers” in the psycho-relational dimension: Perception of Rejection,
23 Perception of Contradictory Affect,
24 Role Reversal (emotional parentification),
25 and Fear.
26 The finalized matrix detailed all 13 constructs across four dimensions and comprised of 22 items and corresponding response options.
The development of the instructions, items, and response options prioritized feasibility. It was grounded in psychological literature on children’s concrete operational thinking and moral judgment, as described by Jean Piaget,¹² as well as on children’s perception of impactful events
13 and their capacity for critical engagement and co-construction of self-report instruments at this age.⁸
Therefore, the IDR-VSD was designed to be playful, easy to read, and quick to complete by schoolchildren. The instrument uses capital letters, clear and intelligible wording,
27 and instructional characters resembling emojis.
28 Events were assessed using a lifetime perspective, and response categories indicating frequency (“number of times”) were applied to items addressing the occurrence of events.
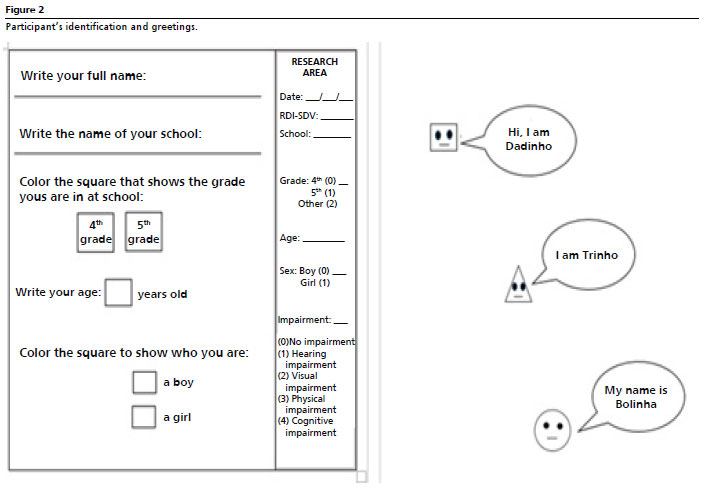
27,29The first version of the IDR-VSD comprised of 22 items and incorporated instructional characters drawn from the school context to facilitate children’s understanding. These included a square character (“
Dadinho”), representing the social dimension; a triangle character (“
Trinho”), associated with items requiring frequency-based response options across the social, psycho-relational, and ecological dimensions; and a circle character (“
Bolinha”), used exclusively for items within the psycho-relation dimension. This initial version was positively evaluated by the expert panel and approved for the pilot testing (Figure 2).
The cognitive interview technique was conducted with 14 students. A larger sample was not feasible due to schools closures during the COVID-19 pandemic. Nevertheless, the COSMIN-recommended information saturation table¹¹ was applied, and this number of participants was sufficient to achieve adequate informational saturation. The interviews were conducted in small groups, in pairs, or individually, depending on the children’s availability. Reinforcing the inclusive purpose of the instrument, participation also included a child with a physical disability (wheelchair user) and mild intellectual disability, who completed the activities with the assistance of a tutor, as well as another child with attention-deficit/hyperactivity disorder (ADHD).
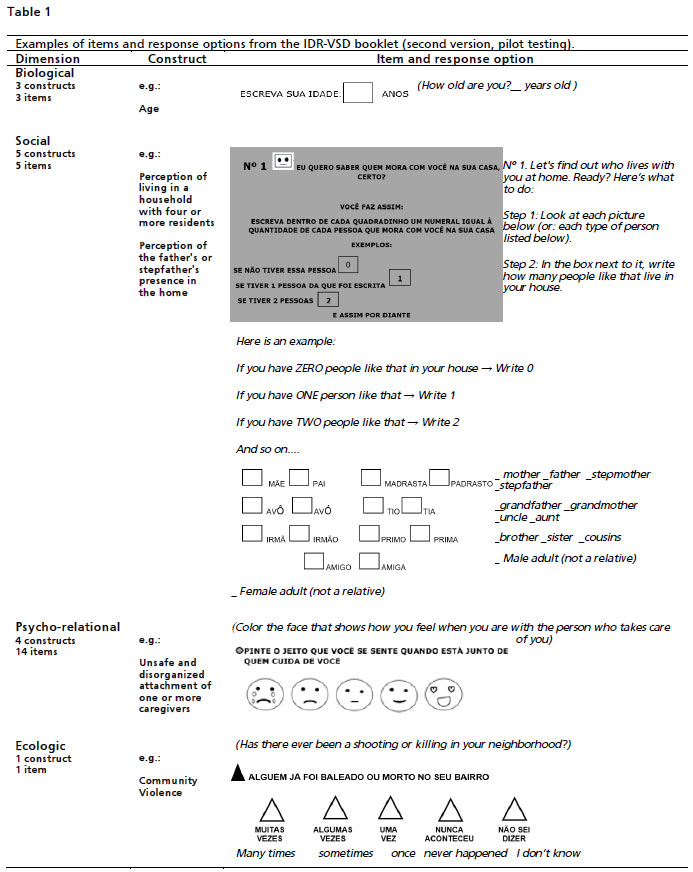
Feedback from the schoolchildren led to improvements in the format of the instrument, resulting in a booklet-style layout in the second (revised) version. Two items addressing the intergenerational transmission of violence were perceived as confusing and therefore,required revisions to the wording. Additional adjustments were made on the layout of the instructions and response options. Table 1 presents examples of the items and corresponding response options from the second (revised) version of the IDR-VSD.
A total of 109 students participated in the pilot test, which was conducted using the second version of the IDR-VSD. The mean time required to complete the questionnaire during the test phase was 15.1 ± 6.4 minutes. The sample comprised 49 boys (45%) and 60 girls (55%), with no statistically significant difference in mean questionnaire scores between girls (23.0±7.4) and boys (23.6±6.6) (
p=0.21). The mean age of the participants was 10.33±1.01 years. According to the teachers’ reports, two of the 109 children had disorders; both had autism spectrum disorder and completed the questionnaire with the support of a specialized school caregiver. Four questionnaires were excluded from the analysis due to missing data on key variables.
Regarding the total scale scores, values ranged from 8 to 43, with a median of 22 and a mean of 23.3 (standard deviation=7.05). The KST indicated a normal distribution of scores (mean=23.3±7.05;
p=0.28). Test–retest reliability was moderate, as indicated by the intraclass correlation coefficient (ICC=0.602; 95%CI=0.48–0.70;
p<0.001). The overall Cronbach’s alpha for the initial 22-item version of the scale, prior to item removal, was 0.602.
Corrected item, total correlations were examined to assess the relationship between each item and the overall scale. Given the complexity of the construct under investigation, items were retained when their exclusion resulted in a reduction of the overall alpha, indicating adequate inter-item correlation. Four items were removed because their exclusion increased internal consistency in the study sample (presence of father or stepfather, number of people in the household, household changes, and distorted self-perception). After retaining 18 items, the overall Cronbach’s alpha increased to 0.654, approaching the COSMIN-recommended threshold of 0.70 for acceptable internal consistency.¹¹
For the test–retest analysis, the mean interval between the test and retest administrations was 14.5±6.4 days. Measurement conditions were comparable across both assessments, and all questionnaires were administered exclusively by the first author. A sufficient subsample of students was available for retesting (n=48).
In the exploratory factor analysis (EFA), Bartlett’s test of sphericity was significant (χ²=320.33;
p<0.001), and The Kaiser–Meyer–Olkin (KMO) measure indicated borderline sampling adequacy (KMO=0.57), with results supporting the suitability of the data for factor analysis (
p<0.001).
Although a sample size of approximately 100 participants (n=105) is often considered acceptable, the KMO is sensitive to the participant-to-item ratio. In this study, the initial 22-item structure resulted in a borderline ratio of approximately 5:1 for a multifactorial model. Moreover, the instrument was intentionally designed with a reduced number of items to ensure feasibility and comprehension, given the age and educational level of the respondents.
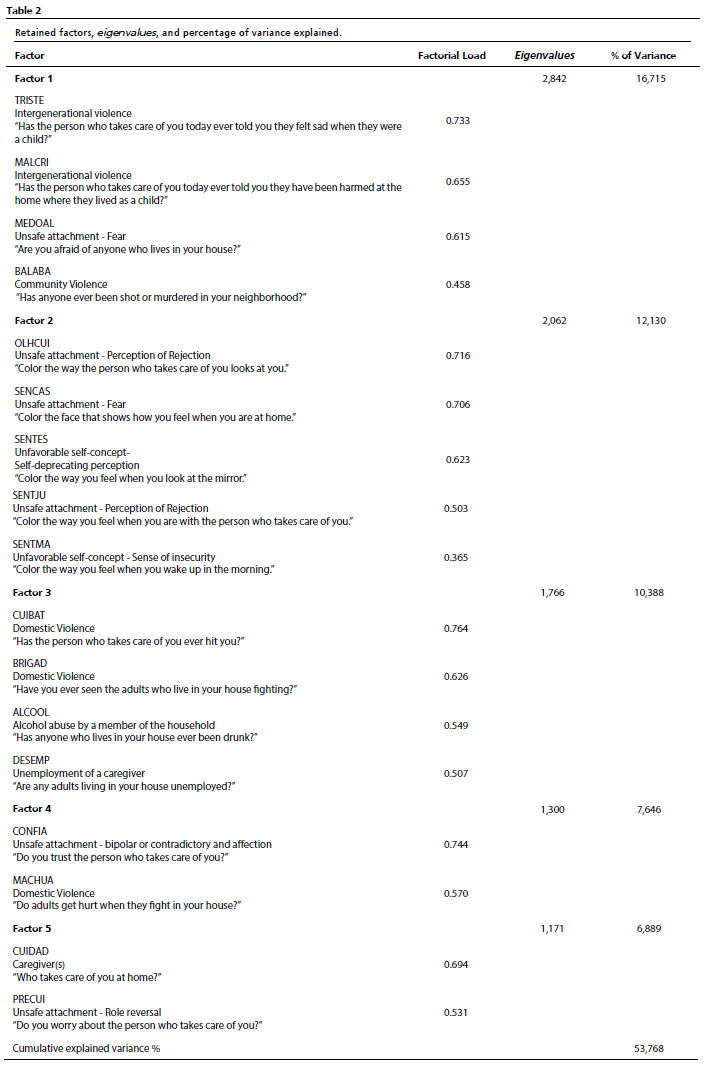
All variables showed communalities (h²) greater than 0.30 and measures of sampling adequacy (MSA) above 0.50, except for three items with MSA values approaching 0.50; two of these were retained due to their substantial communalities. Seventeen items were retained across five factors with
eigenvalues greater than 1, accounting for 53.76% of the total variance explained. The scree plot supported the five-factor solution. A certain degree of cross-loading was observed among items, particularly within correlated domains. This finding is not unexpected, given the complexity of the construct and may reflect conceptual overlap between dimensions rather than a lack of discriminant validity. Most importantly, items showed higher loadings on their primary factors, supporting the overall factorial structure. The retained factors, corresponding
eigenvalues, and percentages of explained variance are presented in Table 2.
The final version of the IDR-VSD comprised 17 items and included adjustments to the response format associated with the character “
Dadinho”, which retained the square symbols, now marked with an “X.”
In our systematic review, no instruments were identified and that exclusively assessed the risk of domestic and sexual violence (DSV) or that targeted a more specific age group aimed to improve the accuracy of risk assessment.
20DiscussionThis study describes the development of the IDR-VSD in accordance with COSMIN requirements, demonstrating satisfactory reliability and an acceptable factorial structure. The Nominal Group Technique (NGT) was intentionally selected to foster in-person, interdisciplinary, and critical dialogue, enabling expert validation of knowledge derived from an extensive scientific literature review and theoretical reflection. The Delphi technique was not adopted, as the study prioritized face-to-face interaction to facilitate immediate exchange of critiques and suggestions regarding the descriptors matrix and theoretical model, allowing for real-time consensus building among experts.
The multidimensional model was designed to approximate the complexity of the relationships among schoolchildren and caregivers, incorporating a temporal perspective and the notion of repetition mediated by intergenerational violence, disorganized insecure attachment, and psychological and physical domestic violence. The blurring of the home external boundaries underscores that the domestic environment is never an isolated unit, but rather embedded within complex and dynamic sociohistorical interactions with multiple interconnected subsystems.
16The IDR-VSD was conceived with an inclusive perspective from its foundational stages, incorporating children with impairment during both the cognitive interview phase and the pilot testing. During the qualitative study and pilot test, we followed Willis
18 and Tay-Lim and Lim
8 recommendations to ensure “listening to their voices” and to minimize researcher influence on the schoolchildren’s responses. The participation of the schoolchildren provided valuable insights that reinforced the need to simplify the language of the instructions, item wording, and response options. These findings also underscored the importance of maintaining the smallest possible number of items, ensuring feasibility, comprehension, and ease of administration.
The reliability of the IDR-VSD should be interpreted in light of the complexity of the construct and the characteristics of the target population. Test–retest reliability, assessed using the intraclass correlation coefficient (ICC), was classified as moderate according to the criteria proposed by Koo and Li.
30 In contrast, internal consistency was evaluated using Cronbach’s alpha, which reached a value close to 0.70. Although COSMIN guidelines¹¹ recommend a minimum alpha of 0.70, Hair
et al.
19 support a threshold of 0.60 for exploratory studies, as in the present research. Overall, these findings suggest acceptable psychometric performance for a pilot study, despite the young age of the respondents and the inclusion of psychosocial domain items.
The proportion of variance explained by the five-factor solution, although slightly below the recommended threshold of 60%, likely reflects the inherent complexity of the construct under investigation and the characteristics of the target population. The risk of sexual domestic violence is a multidimensional and context-dependent phenomenon that cannot be fully captured by a finite set of dimensions and constructs. As a complex object, it necessarily includes elements that extend beyond the theoretical boundaries defined for a specific time, place, and sociocultural context. These findings suggest that the factor structure is promising, but still preliminary. Future studies with a larger sample and the refined version of the instrument are recommended to confirm the factor structure through confirmatory factor analysis and to evaluate the psychometric properties of the scale.
The multidimensional structure identified through the EFA supported the dynamic model of influences on self-formation subsystems proposed in the theoretical framework of this study. Factor 1 reflected an intergenerational and community violence context that influenced attachment patterns. Factor 2 comprised variables more strongly associated with perceived disorganized insecure attachment and an unfavorable self-concept. Factor 3 grouped social dimension variables in conjunction with domestic violence descriptors. Factors 4 and 5 expanded the understanding of domestic violence, capturing its correlations with different manifestations of insecure attachment (Table 2).
The strengths of this study include the use of COSMIN guidelines
11 to ensure transparency and quality in instrument development; the adoption of a specific-age risk measurement construct structured through a theoretical model and descriptors matrix; and the co-construction process involving the participation of both neurotypical and neurodivergent schoolchildren, as well as children with physical impairment. For children with visual or hearing impairment, assistance from a tutor during instrument completion may be required to ensure adequate comprehension and response.
In the systematic review conducted by our group (Bomfim
et al.
20) no instrument was identified that a specific-age risk measurement construct to assess CSA risk in children under 12 years of age.
The next step will be to retest the final version of the IDR-VSD to examine its psychometric properties.
The COVID-19 pandemic imposed substantial restrictions to access schools, limiting the recruitment of a larger number of children and delaying the completion of the study. This study included convenience sampling during the pilot testing phase. Other limitations, although acceptable for pilot studies, included a sample size, only slightly above the minimum recommended threshold of 100 participants for exploratory factor analysis (EFA), as well as a borderline participant-to-item ratio (~5:1). These conditions may have affected factor stability and the precision of factor loadings, potentially resulting in a less stable factor structure and limiting the generalizability of the findings. Therefore, the factor structure identified in this study should be interpreted as preliminary, and further studies with larger samples are recommended to confirm the stability of the model.
Despite these limitations, the IDR-VSD is proposed as a tool to be integrated into systematic child protection strategies aimed to identify situations that require monitoring and risk reduction through organized, preventive, and intersectoral actions. Such integration is expected to include the notification of cases exceeding the SDV score cutoff point, which will be established in subsequent stages of this research. The instrument reinforces the need for effective anti-violence public policies and early family-centered interventions to promote nurturing care. Moreover, this study aligns with Sustainable Development Goal 16 by contributing to the promotion of peaceful and inclusive societies through effective, accountable, and inclusive institutions at all levels.
9This study also addresses the challenge of developing an instrument capable of capturing a complex construct through the active and inclusive participation of schoolchildren aged 9 to 11 years, including children with impairment and neurodevelopmental disorders. The development of the IDR-VSD adhered to COSMIN guidelines
11 and demonstrated favorable indicators of reliability and factor structure.
Exploratory factor analysis identified five interrelated factors that are theoretically coherent with the proposed model and descriptors matrix. Intergenerational violence, disorganized insecure attachment, and physical and psychological domestic violence showed strong intrinsic correlations, reinforcing the multidimensional and dynamic nature of the construct.
The IDR-VSD is a free, community-based instrument designed for large-scale use by a wide range of professionals working with children, including pediatricians, nurses, social workers, psychologists, and teachers. Although, developed in the school context, it is intended to be applicable through diverse settings, such as educational, clinical, and other child-focused care environments. Importantly, the IDR-VSD is not intended to replace the official violence notification form for this age group; rather, it aims to promote and support its timely use by professionals when situations of risk are detected. In addition, the instrument may be particularly useful within a syndemic perspective, as social vulnerability, family violence, and health crises —such as future pandemics — tend to interact and amplify risks for sexual domestic violence.
Future phases of this research will include longitudinal studies to monitor schoolchildren and their families within child protection networks, supporting early risk detection, preventive actions, and coordinated intersectoral responses.
References1. Meinck F, Neelakantan L, Steele B, Jochim J, Davies LM, Boyes M,
et al. Measuring violence against children: a COSMIN systematic review of the psychometric properties of child and adolescent self-report measures. Trauma Violence Abuse. 2023; 24 (3): 1832-47.
2. Stoltenborgh M, van IJzendoorn MH, Euser EM, Bakermans-Kranenburg MJ. A global perspective on child sexual abuse: meta-analysis of prevalence around the world. Child Maltreat. 2011; 16 (2): 79-101.
3. Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V,
et al. Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults: The Adverse Childhood Experiences (ACE) Study. Am J Prev Med. 2019; 56 (6): 774-86.
4. Bradel L, Rosenbaum A, Orcutt H. The Prevalence and Co-Occurrence of the Forms of Violence Against Women. J Aggress Maltreatment Trauma. 2019; 28 (7): 870–87.
5. Saini SM, Hoffmann CR, Pantelis C, Everall IP, Bousman CA. Systematic review and critical appraisal of child abuse measurement instruments. Psychiatry Res. 2019; 272 (November 2018): 106–13.
6. Hughes K, Bellis MA, Hardcastle KA, Sethi D, Butchart A, Mikton C,
et al. The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. Lancet Public Health. 2017; 2 (8): e356–e366.
7. Brasil. Lei [Law] Nº 8.069, de 13 de julho de 1990. Dispõe sobre o Estatuto da Criança e do Adolescente e dá outras providências [Provides on the Child and Adolescent Statute and makes other provisions]. Brasília (DF): DOU 16 de julho de 1990. [access in 2025 Ago 13]. Available from:
http://www.planalto.gov.br/ccivil_03/leis/L8069.htm8. Tay-Lim J, Lim S. Privileging younger children’s voices in research: Use of drawings and a co-construction process. Int J Qual Methods. 2013; 12 (1): 65-83.
9. UNICEF Brasil, Fórum Brasileiro de Segurança Pública. Panorama da violência letal e sexual contra crianças e adolescentes no Brasil (2021-2023). 2
nd ed. São Paulo: UNICEF; 2024 [access in 2026 Apr 20]. 57 p. Available from:
https://www.unicef.org/brazil/media/30071/file/panorama-violencia-letal-sexual-contra-criancas-adolescentes-no-brasil-v04%20(003).pdf.pdf10. Creswell JW. Projeto de Pesquisa: métodos qualitativo, quantitativo e misto [Research design: Qualitative, Quantitative, and Mixed Methods Approaches]. 3
rd ed. Porto Alegre: ARTMED; 2010.
11. Gagnier JJ, Lai J, Mokkink LB, Terwee CB. COSMIN reporting guideline for studies on measurement properties of patient-reported outcome measures. Qual Life Res. 2021 Aug; 30 (8): 2197-218. doi:10.1007/s11136-021-02822-4.
12. Piaget J. Algumas particularidades da compreensão verbal da criança de 9 a 11 anos [Some particularities of verbal understanding in the child between the ages of nine and eleven] In: Piaget J. A Linguagem e o Pensamento da Criança [The Language and Thought of the Child]. 3
rd ed. Rio de Janeiro: Fundo de Cultura; 1973. p. 212-46.
13. Bee H, Boyd D. A criança em desenvolvimento [The developing child]. Porto Alegre: Artmed; 2011.
14. Souza VMG. Pessoas em Minha Vida: o apego e os vínculos afetivos de crianças vítimas de abuso sexual [Pessoas em Minha Vida: o apego e os vínculos afetivos de crianças vítimas de abuso sexual]. [Dissertation]. São Paulo: Universidade de São Paulo; 2012.
15. Bowlby J. Apego [Attachment]. São Paulo: Martins Fontes; 1984.
16. Sameroff A. A unified theory of development: A dialectic integration of nature and nurture. Child Dev. 2010; 81 (1): 6–22.
17. Jones J, Hunter D. Qualitative Research: Consensus methods for medical and health services research. Bmj. 1995; 311 (7001): 376.
18. Willis G. Special Applications of Cognitive Interviewing. Cogn Interviewing. 2011; 176-206.
19. Hair JF Jr, Black WC, Babin BJ, Anderson RE. Análise multivariada de dados [Multivariate Data Analysis]. 6
th ed. Porto Alegre: Bookman; 2009.
20. Bomfim KDX, Leite URL, Goes PSA. A systematic review of the measurement properties of self-report screening tools to detect risk or exposure to child sexual abuse for children under 12. Heliyon. 2023; 9 (9): e20366.
21. Assis SG, Avanci JQ. Labirinto de espelhos [Maze of mirrors]. Rio de Janeiro: Editora FIOCRUZ; 2004.
22. Tamayo A. EFA: Escala Fatorial de Autoconceito. Arquivos Brasileiros de Psicologia. 1981; 33 (4): 87-102.
23. Ruddle A, Pina A, Vasquez E. Domestic violence offending behaviors: A review of the literature examining childhood exposure, implicit theories, trait aggression, and anger rumination as predictive factors. Aggression and Violent Behavior. 2017; 34, 154-65.
24. Zimmer-Gembeck MJ, Webb HJ, Pepping CA, Swan K, Merlo O, Skinner EA,
et al. Review: Is Parent Child Attachment a Correlate of Children’s Emotion Regulation and Coping? Int J Behav Dev. 2017; 41 (1): 74-93.
25. Fitzgerald MM, Schneider RA, Salstrom S, Zinzow HM, Jackson J, Fossel R V. Child Sexual Abuse, Early Family Risk, and Childhood Parentification: Pathways to Current Psychosocial Adjustment. J Fam Psychol. 2008; 22 (2): 320-4.
26. Dixon KJ. The effect of family violence on peer and partner violence patterns: An examination of self-concept as a mediating mechanism. ProQuest Diss Theses. 2016; 156.
27. Streiner DL, Norman GR, Cairney J. Health measurement scales-a practical guide to their development and use. 5
th ed. Oxford, United Kingdom: Oxford Press; 2015.
28. Fane J, MacDougall C, Jovanovic J, Redmond G, Gibbs L. Exploring the use of emoji as a visual research method for eliciting young children’s voices in childhood research. Early Child Dev Care. 2018; 188 (3): 359-74.
29. Pasquali L. Instrumentos psicológicos: manual prático de elaboração [Psychological instruments: practical handbook of elaboration]. Brasília: LabPAM; 1999.p: 37-71.
30. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016; 15 (2): 155-63.
Authors’ contributionBomfim KDX: conceptualisation, data curation, formal analysis, methodology, project administration, resources, visualisation, writing – original draft, and writing, review & editing.
Leite UR: co-advisor of the research, was present in data collection, analysis and manuscript preparation and review.
Goes PSA: research advisor, was present in qualitative and quantitative analysis, software and manuscript preparation and review.
All authors approved the final version of the article and declare no conflicts of the interest.
Data availabilityThe datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Received on September 3, 2025
Final version presented on April 20, 2026
Approved on April 22, 2026
Associated Editor: Lygia Vanderlei


 ; Umbelina do Rego Leite2
; Umbelina do Rego Leite2