ABSTRACT
OBJECTIVES: to evaluate outcomes in pregnant patients diagnosed with cancer compared to pregnant women without cancer.
METHODS: a systematic review with meta-analysis was conducted, including studies from PubMed, Lilacs, Scielo, and Cochrane databases, published between 2019 and 2024, in Portuguese, English, or Spanish, and containing a control group. The search used descriptors combined with the Boolean operators AND and OR, covering terms related to pregnancy and neoplasms. Unretrievable articles, case reports, case series, or expert commentaries were excluded. The study protocol was registered in the PROSPERO database with the number CRD42024534208. Risk of bias for each study was assessed using the ROBINS-I guidelines, and results were presented descriptively.
RESULTS: Nine observational studies were included, a total of 13,316 pregnant women with cancer. The risk of confounding and selection bias was high. Findings showed an increased risk of maternal death (OR=82.11; 95%CI=20.27-332.69), maternal blood transfusion (OR=4.45; 95%CI=3.48-5.68), and cesarean (OR=1.96; 95%CI= 1.61-2.38).
CONCLUSION: pregnant women with cancer have increased maternal morbidity and mortality. Due to study heterogeneity and high risk of bias, these findings should be interpreted with caution. Multidisciplinary care and more robust research are necessary.
Keywords:
Neoplasias malignas, Morte materna, Complicações na gravidez, Revisão sistemática, Meta-análise
RESUMO
OBJETIVOS: avaliar resultados gestacionais de pacientes diagnosticadas com câncer na gestação comparados com gestantes sem câncer.
MÉTODOS: foi realizada uma revisão sistemática com meta-análise, incluindo estudos em bancos de dados PubMed, Lilacs, SciELO e Cochrane, publicações entre 2019 e 2024 com artigos em português, inglês ou espanhol que continham grupo controle. A busca utilizou descritores combinados pelos operadores booleanos AND e OR, abrangendo os termos relacionados a gestação e neoplasias. Foram excluídos artigos não recuperados, relatos ou série de casos ou comentários de especialistas. O protocolo foi registrado no banco de dados PROSPERO sob número CRD42024534208. O risco de viés de cada estudo foi avaliado pelas diretrizes ROBINS-I, e os resultados foram apresentados de forma descritiva.
RESULTADOS: foram incluídos 9 estudos observacionais, com um total de 13.316 gestantes com câncer. Os riscos de viés de confusão e seleção foram altos. Os resultados mostraram maior risco de morte materna (OR=82,11; IC95%=20,27–332,69), transfusão sanguínea materna (OR=4,45; IC95%=3,48–5,68) e cesariana (OR=1,96; IC95%= 1,61–2,38).
CONCLUSÃO: mulheres com câncer associado à gestação apresentam maior morbimortalidade materna. Devido à heterogeneidade dos estudos e alto risco de viés, os achados devem ser interpretados com cautela. Cuidados multidisciplinares e pesquisas mais robustas são necessários.
Palavras-chave:
Neoplasias malignas, Morte materna, Complicações na gravidez, Revisão sistemática, Meta-análise
IntroductionMalignant neoplasms have become the second leading cause of death in women of reproductive age and can occur during pregnancy-puerperal cycle. Although the incidence of cancer during pregnancy may be low, recent studies indicate an increase over time, complicating approximately 1 in every 1,000 pregnancies.
1-4Age alone is considered a significant risk factor for several diseases, including cancer.
5 There is a trend for women to become pregnant later in life, which influences the increase in cases of the disease.
5Cancer associated with pregnancy is traditionally defined as a diagnosis of malignancy occurring 3 months before an abortion, 9 months before delivery, or up to 1 year after the end of the pregnancy,
1,6 although this definition may be controversial. In clinical practice, any cancer concomitant with pregnancy - whether it is primary, recurrent, or previously diagnosed - represents a significant complication of pregnancy and maternal prognosis. One of the main challenges is late diagnosis, which often occurs in more advanced stages of the disease, since symptoms related to malignancy (fatigue, vaginal bleeding, anemia, abdominal pain, and breast lumps) are attributed to physiological changes in pregnancy and are not immediately investigated.
1-3Breast cancer, lymphoma, leukemia, melanoma, and cervical cancer are the most frequently diagnosed, corresponding to the most common subtypes of neoplasia in women of reproductive age.
1-3Managing the disease during pregnancy is challenging and is associated with a worse prognosis, requiring approaches that benefit the pregnant woman with the least possible impact on the fetus.
6 In view of this, it may be necessary to decide between terminating the pregnancy to begin treatment or continue the pregnancy. When pregnancy is maintained, options become more limited, and there is a risk that diagnostic, staging, and therapeutic methods may negatively affect the fetus in development.
3The available studies are diverse and often have conflicting results, which can influence conclusions, analyses, and clinical decisions. Therefore, a synthesis of the available evidence regarding maternal outcomes of patients diagnosed with cancer during pregnancy can help better understand these data, assist in providing adequate information to families undergoing a cancer diagnosis during pregnancy, and in proposals for public policies and adequate care for these patients.
In this matter, the objective of this systematic review and meta-analysis is to evaluate maternal outcomes (maternal death, blood transfusion, ICU admission, cesarean section) in patients diagnosed with cancer during pregnancy compared to pregnant women without cancer.
MethodsThis is a systematic literature review and meta-analysis. The study protocol was registered in the PROSPERO database of systematic reviews (protocol number CRD42024534208). The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020
7 and MOOSE
8 guidelines were followed.
The inclusion criteria were: observational studies of the Cross-sectional, Cohort, and Case-control types; publications such as, original articles or conference presentations; with sufficient maternal data for quantitative analysis; with a control group; between 2019 and 2024; in Portuguese, English, or Spanish. The exclusion criteria were: articles not retrieved; reports or case series or experts' comments.
A systematic search was performed using the PubMed, Lilacs, SciELO, and Cochrane databases. The search was conducted between August 29 and 31, 2024. The time frame between 2019 and 2024 was defined to capture the most recent analyses with appropriate analytical methodologies and a greater likelihood of including contemporary data on the characteristics researched, since both the profile of the obstetric population and the oncological and clinical approach have changed over time.
The terms used for the search were: ("Pregnant Women" OR Pregnan* OR 'Pregnancy' OR Gestation* OR "Prenatal Care" OR "Prenatal" OR Perinata*) AND ("Neoplasms" OR Neoplasm* OR Cancer* OR Neoplasia* OR Tumor*) AND ("Pregnancy Complications, Neoplastic" OR "Pregnancy Complications" OR "Adverse Birth Outcomes" OR "Adverse Outcomes" OR "Adverse Outcome" OR Complica*).
The abstract selection process was performed on the Rayyan platform. Initially, the retrieved records were entered into the platform, which was also used for automatic duplicate removal. Subsequently, two independent reviewers read and selected the abstracts based on the previously established criteria. After this step, the full texts of the selected articles were retrieved and read in full by the two independent researchers. Articles that did not meet the inclusion criteria were excluded, with the reasons for their exclusion being recorded. Studies that used the same databases were also identified and excluded from the analysis to avoid duplication of information. In cases of disagreement between the researchers, decisions were discussed and resolved in a research group meeting.
The data were extracted from the publications by two researchers, who worked together (not independently). In cases of doubt or difficulty in data extraction, the issues were discussed in a group and, when necessary, resolved with the help of the project coordinator.
To organize the information, a spreadsheet was created in Excel containing all the previously defined variables of interest. The extracted data were entered directly into this spreadsheet. Due to the diversity and heterogeneity of the included studies, some specific information could not be retrieved.
For this study, maternal and delivery outcomes were presented. Due to the heterogeneity of the neoplasms included in the studied populations, it was not possible to perform specific analyses by subgroup, such as cancer type, treatment, or follow-up. Studies comparing different therapies or follow-up strategies for neoplasms were included; however, the extracted data considered only the general outcomes of patients diagnosed with cancer. For this analysis, studies with a control group composed of pregnant women, women in labor, and puerperal women without cancer were used. Descriptive studies and those whose control group consisted of non-pregnant people with cancer were not included.
The following outcomes were analyzed: maternal death, maternal blood transfusion, maternal ICU admission, and cesarean sections. Missing information, information provided only as a percentage (without absolute numbers), or unclear information was not included in each analysis.
Studies that used patients without cancer as control were analyzed using odds ratio (OR) and the Mantel-Haenszel method with random effect measurement. The analyses were performed using the REVMAN program.
9The risk of bias in each study was assessed using the ROBINS-I guidelines, as these were observational studies without intervention. To assess publication bias, funnel graphs were made of the studies with a control group, considering the Log of Relative Risk and the respective standard error for each study. The certainty of the evidence was assessed using the GRADE (Grading of Recommendations, Assessment, Development and Evaluations) method.
10There was no financial support for this study, and the authors have no conflicts of interest.
ResultsA total of 9 articles were included in the review, with a total of 13,316 pregnant women with cancer. The flowchart describing the selection of articles is shown in Figure 1. One article was not retrieved even after the attempt of contacting the author by email.
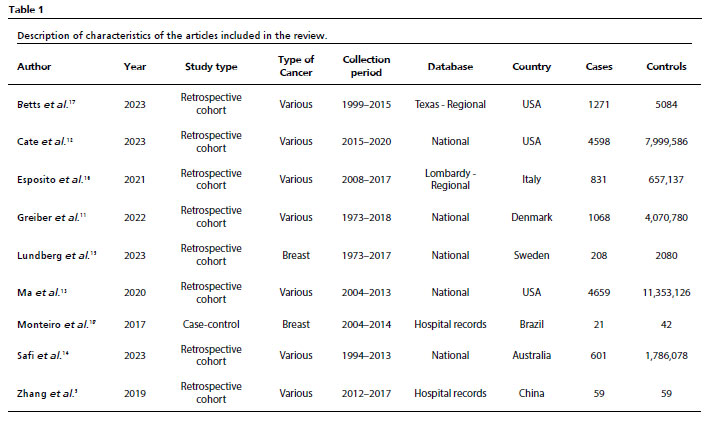
The characteristics of the articles are summarized in Table 1. The selected studies contained data collected between 1973 and 2020, and the databases and selection of subjects and controls have different methodologies. Four studies used databases from the population of Denmark,
11 the United States,
12,13 and Australia,
14 and their controls were all pregnant women without diagnosis of malignant neoplasms.
11-14 Lundberg
et al.15 also used a national database (from Sweden), but the controls were matched by age, at a ratio of 1 patient with cancer to 10 controls without cancer. Esposito
et al.
16 matched each pregnant woman with cancer with 4 pregnant women without cancer at the same age and year of delivery. Similarly, Betts
et al.17 used a regional database from the United States and also matched each live birth to a patient with cancer with four patients without cancer. Two studies were conducted using hospital records, one in Brazil
18 and the other in China.
5 Monteiro
et al.
18 matched each case with two pregnant women at the same age without cancer, and Zhang
5 matched each pregnant woman with cancer with one without cancer.
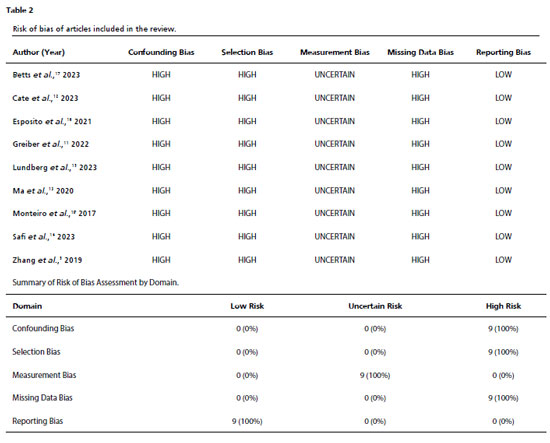
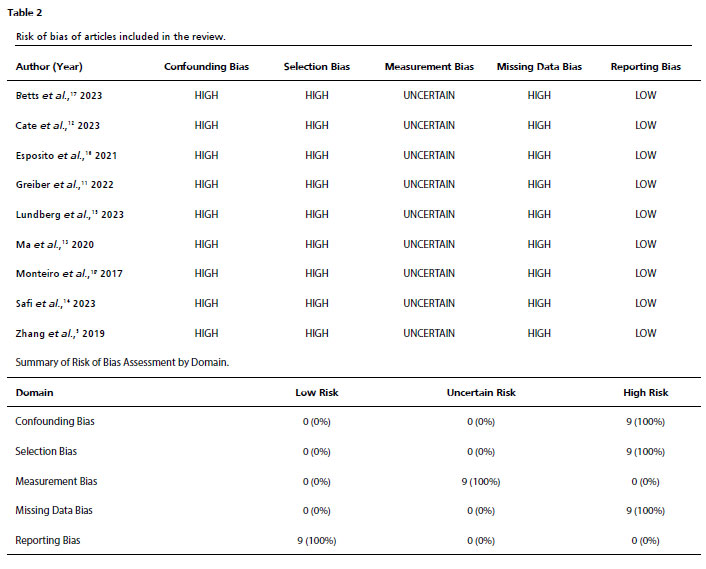
Table 2 describes the risk of bias in each study, considering confounding bias, selection bias, measurement bias, missing data bias, and reporting bias. The risk is similar across studies for several reasons. Among them, the methodology of the studies analyzed stands out, as they are observational and more prone to intrinsic biases, such as confounding, selection, and measurement biases. In addition, the authors of all studies collected information from hospital records or international, national, or regional databases and are prone to missing data or incorrect data collection. This high risk of bias should be taken into account when interpreting the results. The results presented by the studies are aligned with their objectives and were reported transparently, with no evidence of outcome selection based on statistical significance.
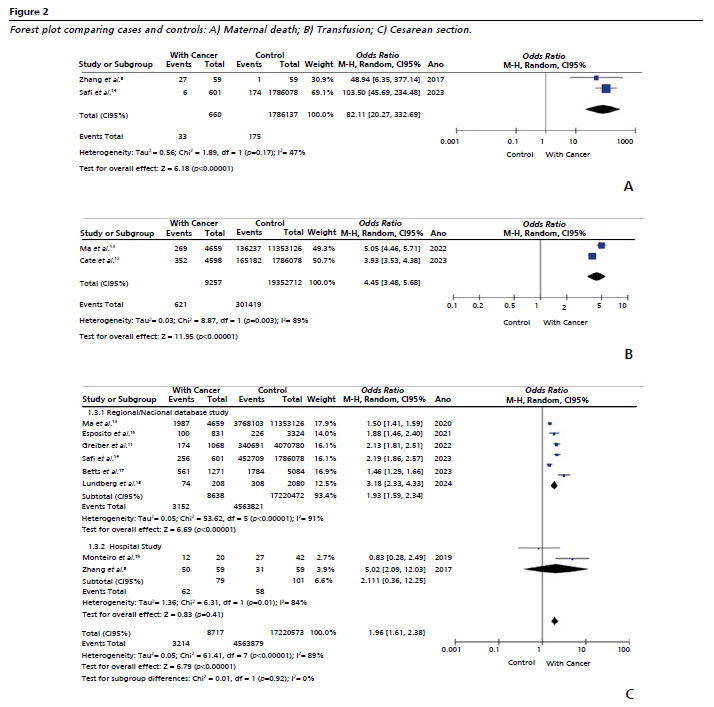
Two studies analyzed maternal deaths with a comparison group, with a total of 660 cancer patients and 33 deaths. Although the number of studies is limited, the robust sample size justifies the meta-analysis. The results are shown in Figure 2A. Data on deaths of patients in the control group of the study by Safi
et al.14 were retrieved by consulting the database cited in the supplementary data presented in the article. The OR for maternal mortality was 82.11 (95% CI=20.27–332.69), with statistical significance for women with cancer.
The level of heterogeneity between the two studies is moderate (I
2=47%,
p= 0.17). The quality of evidence, assessed by the GRADE system, was classified as low due to the methodology of the studies (observational) and the possible biases of each study.
The need for maternal blood transfusion was reported in two studies, and the results of the analysis are described in Figure 2B. As in the case of maternal death, the number of studies is small, but inclusion in the meta-analysis is justified by the sample size and number of events. Cancer patients had an OR=4.45 (95%CI=3.48–5.68) of receiving a blood transfusion.
In this analysis, the heterogeneity of the studies is high (I
2=89%,
p=0.003). The quality of evidence is considered low, mainly due to the heterogeneity of the studies and the observational methodology, which leads to a high probability of bias.
The cesarean section rate was presented in eight studies, six of which were based on regional or national databases and two on hospital medical records. It should be noted that the studies cover different period - with cases collected since 1973 in the Swedish
15 and Danish
11 studies and also different obstetric realities with very different cesarean rates in people without cancer, which already represents an important confounding bias for this variable.
The results of the meta-analysis comparing studies based on regional or national databases showed an OR of 1.93 (95%CI=1.59–2.34) and for studies based on hospital records 2.11 (95%CI=0.36–12.25), therefore without statistical significance. The analysis of all studies indicates a significant increase in the chance of cesarean section among people with malignant neoplasms – OR of 1.96 (95%CI=1.61–2.38) (Figure 2C).
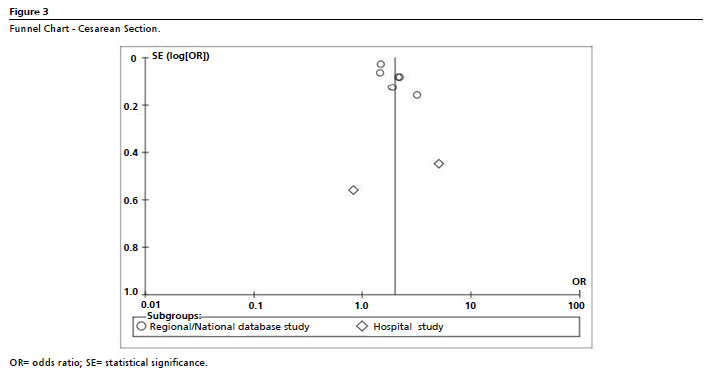
Even with the division of studies into subgroups, the analyses revealed high heterogeneity among the studies, making it difficult to generalize. However, no significant publication bias was observed in the funnel plot (Figure 3).
Although this result presents a lower possibility of outcome measurement bias, the possible loss of data and high heterogeneity among the studies reduces the quality of the evidence, classifying it as low.
None of the selected studies presented data on maternal admission to the ICU.
DiscussionIn this meta-analysis, nine studies were selected and data of more than 13,000 complicated pregnancies due to cancer in seven countries were included. In three studies
12,16,17 breast cancer was the most prevalent, and this type of cancer was also the only one studied in two of the studies included in this review.
15,18 Other types of cancer, such as skin, cervical, and hematological cancers, were also cited as the most common,
5,11,13,14 which corroborates the data described by Eastwood
1 and Amant.
2The available data suggest that the risk of maternal death may be more than 80 times higher in pregnant women diagnosed with cancer, although this estimate should be interpreted with caution due to the heterogeneity of the studies and the small number of studies analyzed. In addition to mortality associated to neoplasm itself, obstetric complications may be more frequent in women with malignant neoplasms, such as the possibility of puerperal infections in patients undergoing chemotherapy,
18,19 the risk of hypertensive conditions in people with cancer,
20 and the risk of bleeding related to cervical cancer
21 and myeloproliferative neoplasms.
22 Unfortunately, we cannot determine whether the increased risk of death is due to complications related to cancer during pregnancy or its treatment, as the causes of death were not described in the studies analyzed. It should be noted that although the I
2 of the meta-analysis is moderate, the studies included are heterogeneous, as one refers to regional data from a study in Australia
14 and another to hospital records in China
5. Socioeconomic conditions, maternal health care, and access to treatment for neoplasms are different in both countries.
Among cancer patients, pregnancy may increase the risk of death, a fact that we were unable to prove in this research, since we only have two studies evaluating the mortality rate, and comparing pregnant and non-pregnant women with cancer was not the scope of this study. One of the factors that led to this increase in mortality is associated with delays in starting treatment, since in some cases diagnosis, staging, and treatment are postponed due to confusion with pregnancy symptoms and/or risks to the fetus.
1-3 As discussed in a previous meta-analysis, for every 4 weeks of delay in treatment, the risk of death increases.
23 In the case of breast cancer, for example, a 12-week delay is associated with a 17% increase in mortality.
23 Zhang
et al.
5 also describe that pregnant women who received chemotherapy had a significantly lower mortality rate than pregnant women who chose not to receive treatment. Another hypothesis would be that the diagnosis made during pregnancy is late, at a time when the disease is more widespread and has lower cure rates. As assessed by Walters
et al.,
24 worse maternal outcomes occurred in 64% of cases where cancer was diagnosed during pregnancy or within 12 months after delivery.
The chance of blood transfusion was more than four times higher for the analyzed cancer patients, although this finding is based on only two studies with different care contexts. One hypothesis for this increased risk is that myeloproliferative neoplasms are associated with an increased risk of bleeding, which can lead to episodes of hemorrhage during pregnancy, childbirth, or ouerperal period.
22 Ma
et al.
13 reiterate the increased risk of blood transfusion in cancer patients, but do not describe a significant difference between hematological and non-hematological malignancies. In a study conducted in the United States,
25 a significantly higher chance of blood transfusion was observed in patients with thyroid cancer, which may be due to the association of anemia with thyroid diseases.
26,27Women diagnosed with cancer during pregnancy were more likely to undergo cesarean section; however, the high heterogeneity among studies limits the generalization of this finding. One possible explanation is that the responsible healthcare teams are more likely to plan the timing of birth to reduce any delay in treatment or even to perform therapeutic interventions.
24 Vaginal delivery is generally avoided in patients with cervical cancer, for example, due to the risks of hemorrhage, tumor rupture, and disease spread.
16,23,26 It is noteworthy that, in the only Brazilian study,
18 patients without cancer had more cesarean sections than patients with neoplasia. The authors did not presente any discusstion about this fact, but the high rate of cesarean sections in the country may be a justification.
28There is a gap in the literature and current guidelines regarding the optimal timing of planned cesarean sections for pregnant women diagnosed with cancer. A multidisciplinary approach involving experienced obstetricians, neonatologists, and oncologists is necessary to ensure the best outcomes, optimizing the health of both the woman and the newborn.
14This review and meta-analysis synthesizes the available evidence on maternal outcomes in women diagnosed with cancer during pregnancy, suggesting an association with increased risk of maternal mortality, blood transfusion, and cesarean section, a consistent result with what is expected given the severity of the disease and its impact on the patient, although the quality of evidence is limited by the heterogeneity of the studies and the risk of bias. The findings point to a significant increase in morbidity and mortality in the pregnant population, reinforcing the need to consider this group of patients as high gestational and clinical risk, requiring specific care. For clinical practice, the data collected here, despite their limitations, suggest the need to monitor this population in tertiary centers, with access to blood products and surgical care. A strength of this study was the large number of participants and cases of pregnancy-associated cancer extracted from large studies based on regional, national, and international databases.
The main limitation of this study is the high heterogeneity of the articles analyzed. It should also be noted that the studies included in this review cover a wide time interval (1973 to 2020) and were conducted in different settings and health systems. This diversity of historical, geographical, and healthcare contexts further compromises the comparability of the data and increases the risk of confounding factors. In addition, due to the methodology of the studies found, the risk of confounding and selection bias may compromise the results. It is also observed that the vast majority of the studies are from developed countries, with only one study conducted in Brazil
18 and one in China,
5 which represents an important geographical and epidemiological bias, especially in relation to the most prevalent type of neoplasm, such as cervical cancer.
For maternal mortality and the necessity for blood transfusions, only two studies were analyzed, which prevents the use of the funnel chart. In the case of the cesarean section rate, although the analysis included eight studies, the high heterogeneity and diversity of data sources (population and hospital databases) also reduce the robustness of the assessment. Therefore, despite the absence of obvious asymmetries in the funnel charts, the presence of publication bias cannot be completely ruled out.
The absence of subgroup analysis, considering the different types of cancer included, also hinders the interpretation of results and limits the applicability of the findings to individual clinical contexts.
Maternal admission to the ICU was an outcome of interest in this review; however, none of the included studies presented data related to this outcome, which also limits the understanding of the clinical severity of pregnant women with cancer.
Population studies
11-17also present the possibility of subject selection bias and measurement of effects. For this reason, the quality of evidence we were able to extract from the analyzed studies is low.
Further researches on cancer during pregnancy are necessary, with more defined standards to add new data and results in a systematic way, especially related to the types of neoplasia. In this matter, specific care protocols can be formulated for this population.
Final considerationsThe data analyzed suggest that women diagnosed with cancer during pregnancy and the pregnancy-postpartum cycle may experience a significant increase in maternal morbidity and mortality. The studies included in this systematic review and meta-analysis indicate a higher risk of maternal death, maternal blood transfusion, and cesarean section. However, these findings should be interpreted with caution, since the studies included are mostly observational, highly heterogeneous, and at high risk of bias, which limits the robustness of the available evidence. Further researches are necessary to understand the mechanisms involved in this increased risk and to define optimal approaches for managing these patients in different gestational contexts.
References1. Eastwood-Wilshere N, Turner J, Oliveira N, Morton A. Cancer in Pregnancy. Asia Pac J Clin Oncol. 2019; 15 (6): 96–308.
2. Amant F, Han SN, Gziri MM, Vandenbroucke T, Verheecke M, Van Calsteren K. Management of cancer in pregnancy. Best Pract Res Clin Obstet Gynaecol. 2015; 29 (5): 741–53.
3. Jeremic K, Stefanovic A, Dotlic J, Kadija S, Kontic O, Gojnic M,
et al. Cancer during pregnancy – clinical characteristics, treatment outcomes and prognosis for mothers and infants. J Perinat Med. 2018; 46 (1): 35–45.
4. Milosevic B, Likic Ladjevic I, Dotlic J, Beleslin A, Mihaljevic O, Pilic I,
et al. Cancer during pregnancy: Twenty-two years of experience from a tertiary referral center. Acta Obstet Gynecol Scand. 2024; 103 (4): 716–28.
5. Zhang X, Meng X, Chen Y, Leng SX, Zhang H. The Biology of Aging and Cancer: Frailty, Inflammation, and Immunity. Cancer J. 2017; 23 (4): 201–5.
6. Oliveira MDMS, Salgado CDM, Viana LR, Gomes-Marcondes MCC. Pregnancy and Cancer: Cellular Biology and Mechanisms Affecting the Placenta. Cancers. 2021; 13 (7): 1667.
7. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD,
et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; n71.
8. Brooke BS, Schwartz TA, Pawlik TM. MOOSE Reporting Guidelines for Meta-analyses of Observational Studies. JAMA Surg. 2021; 156 (8): 787.
9. The Cochrane Collaboration. Review Manager (RevMan) [Computer program]. Version 5.4. Copenhagen: The Nordic Cochrane Centre; 2020.
10. Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P,
et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008; 336 (7650): 924-6.
11. Greiber IK, Viuff JH, Mellemkjær L, Hjortshøj CS, Lidegaard Ø, Storgaard L,
et al. Cancer in pregnancy and the risk of adverse pregnancy and neonatal outcomes: A nationwide cohort study. BJOG Int J Obstet Gynaecol. 2022; 129 (9): 1492–502.
12. Cate JJM, Sundermann AC, Campbell AIK, Sugrue R, Dotters-Katz SK, James AH,
et al. High rates of venous thromboembolism among deliveries complicated by cancer. J Thromb Haemost. 2023; 21 (10): 2854–62.
13. Ma KK, Monsell SE, Chandrasekaran S, Gadi VK, Gammill HS. Cancer and Pregnancy: National Trends. Am J Perinatol. 2022; 39 (02): 144–53.
14. Safi N, Li Z, Anazodo A, Remond M, Hayen A, Currow D,
et al. Pregnancy associated cancer, timing of birth and clinical decision making—a NSW data linkage study. BMC Pregnancy Childbirth. 2023; 23 (1): 105.
15. Lundberg FE, Gkekos L, Rodriguez-Wallberg KA, Fredriksson I, Johansson ALV. Risk of obstetric and perinatal complications in women presenting with breast cancer during pregnancy and the first year postpartum in Sweden 1973–2017: A population-based matched study. Acta Obstet Gynecol Scand. 2024; 103 (4): 684–94.
16. Esposito G, Franchi M, Dalmartello M, Scarfone G, Negri E, Parazzini F,
et al. Obstetric and neonatal outcomes in women with pregnancy associated cancer: a population-based study in Lombardy, Northern Italy. BMC Pregnancy Childbirth. 2021;21(1):31.
17. Betts AC, Shay LA, Lupo PJ, Pruitt SL, Roth ME, Allicock MA,
et al. Adverse birth outcomes of adolescent and young adult women diagnosed with cancer during pregnancy. JNCI J Natl Cancer Inst. 2023; 115 (6): 619–27.
18. Monteiro DLM, Nunes CL, Rodrigues NCP, Antunes CA, Almeida EM, Barmpas DBS,
et al. Fatores associados ao câncer de mama gestacional: estudo caso-controle. Ciênc Saúde Colet. 2019; 24 (6): 2361–9.
19. Huang X, Zhang C, Zhu J, Li Y, Tang J. Influence of cancer in pregnancy on obstetric and neonatal outcomes: an observational retrospective cohort study. J Gynecol Oncol. 2024; 35 (6): e74.
20. Souza VBD, Silva EN, Ribeiro ML, Martins WDA. Hypertension in Patients with Cancer. Arq Bras Cardiol. 2015; 104 (3): 246-52.
21. Fotheringham P, Safi N, Li Z, Anazodo A, Remond M, Hayen A,
et al. Pregnancy-associated gynecological cancer in New South Wales, Australia 1994–2013: A population-based historical cohort study. Acta Obstet Gynecol Scand. 2024; 103 (4): 729–39.
22. Landtblom AR, Andersson TML, Johansson ALV, Wendel SB, Lundberg FE, Samuelsson J,
et al. Pregnancy and childbirth outcomes in women with myeloproliferative neoplasms—a nationwide population-based study of 342 pregnancies in Sweden. Leukemia. 2022; 36 (10): 2461–7.
23. Hanna TP, King WD, Thibodeau S, Jalink M, Paulin GA, Harvey-Jones E,
et al. Mortality due to cancer treatment delay: systematic review and meta-analysis. BMJ. 2020; m4087.
24. Walters B, Midwinter I, Chew-Graham CA, Jordan KP, Sharma G, Chappell LC,
et al. Pregnancy-Associated Cancer: A Systematic Review and Meta-Analysis. Mayo Clin Proc Innov Qual Outcomes. 2024; 8 (2): 188–99.
25. Spiegel E, Spence AR, Czuzoj-Shulman N, Abenhaim HA. Pregnancy outcomes after thyroid cancer. J Perinat Med. 2019; 47 (7): 710–6.
26. M'Rabet-Bensalah K, Aubert CE, Coslovsky M, Collet T, Baumgartner C, Den Elzen WPJ,
et al. Thyroid dysfunction and anaemia in a large population-based study. Clin Endocrinol (Oxf). 2016; 84 (4): 627–31.
27. Padovani RP, Tuttle RM, Grewal R, Larson SM, Boucai L. Complete Blood Counts are Frequently Abnormal 1 Year after Dosimetry-Guided Radioactive Iodine Therapy for Metastatic Thyroid Cancer. Endocr Pract. 2014; 20 (3): 213–20.
28. Brasil. Ministério da Saúde. Sistema de Informações sobre Nascidos Vivos (SINASC). [
Internet]. Brasília (DF): DATASUS; 2020 [access in 2025 Jan 8]. Available from:
http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sinasc/cnv/nvuf.defAuthors' contributionJaime Prazeres Y: Data curation (Equal), Methodology (Equal), Writing - original draft (Equal), Writing - review and editing (Equal).
Cristiane Hintz M: Data curation (Support), Writing - review and editing (Support)
Oliveira Pires R and Trapani Júnior A: Supervision (Support), Writing - review and editing (Support)
Knobel K: Formal analysis (Equal), Methodology (Equal),
Supervision (Equal), Validation (Equal), Visualization (Equal), Writing - original draft (Equal), Writing - review and editing (Equal).
All authors approved the final version of the article and declare no conflict of interest.
Data availabilityThe entire dataset supporting the results of this study has been published in the article itself.
Received on February 26, 2025
Final version presented on December 24, 2025
Approved on January 7, 2026
Associated Editor: Alex Sandro Souza


 ; Micheli Cristiane Hintz2
; Micheli Cristiane Hintz2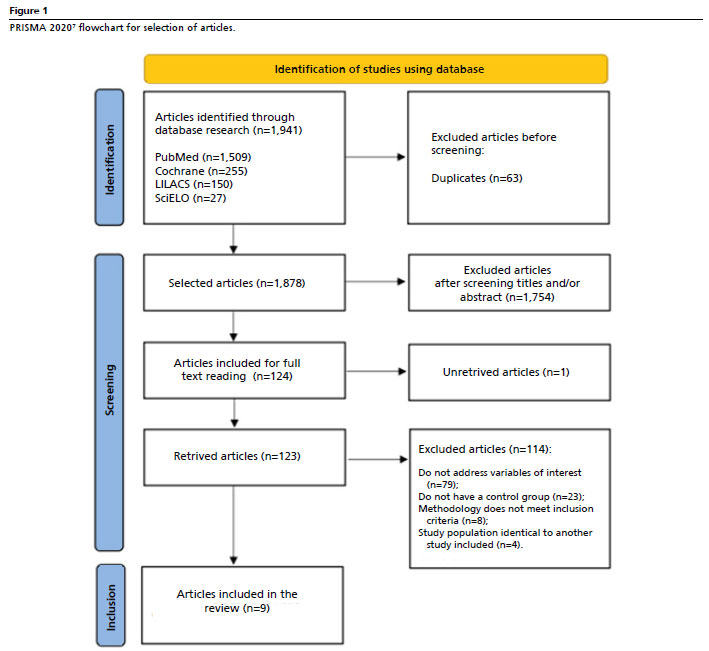






 Ler em português
Ler em português