ABSTRACT
OBJECTIVES: to evaluate changes in breast cancer care among women assisted at a public hospital in Paraíba, Brazil, during the COVID-19 pandemic.
METHODS: retrospective cohort of women using the Sistema Único de Saúde (SUS) (Brazilian Public Health Service) at Hospital Napoleão Laureano (PB), and were diagnosed with in situ or invasive ductal carcinoma in the pre-pandemic (2017-2018) and pandemic (2020) periods. Sociodemographic, clinical and care-related data were collected. Differences between periods were assessed using chi-square or Fisher's exact test for categorical variables and Student's t or Mann-Whitney tests, for continuous variables (p<0.05).
RESULTS: among 218 women included, 114 were treated before the pandemic and 104 during. Most cases were palpable tumors and invasive carcinoma. Mastectomy was the predominant procedure, with immediate reconstruction in 24.8%. The interval between histopathological diagnosis and the first consultation with a specialist increased during the pandemic (p=0.04), and few women outside the capital could access the service (RR=0.63; 95%CI= 0.4-0.9; p=0.01). Delays on the appointment and abandonment of treatment were also higher during the pandemic, whereas immediate breast reconstruction decreased.
CONCLUSION: the pandemic hindered breast cancer care, increasing delays, interruptions of treatment, and reducing immediate reconstructions. These findings highlight the vulnerability of patients dependent of the public health services during health crises.
Keywords:
Neoplasias da mama, SARS-CoV-2, Pandemia, Diagnóstico tardio, Tempo para o tratamento
IntroductionBreast cancer is the most common type of cancer among the female population, representing the fifth cause of death from cancer in general and the most frequent cause of cancer-related death in women.
1 Early detection, along with treatment at initial stages, constitutes the best strategy in reducing mortality of the disease.
Currently, mammography is the imaging technique of choice for breast cancer screening and it has been well-established that mammography screening is effective for women 50 to 74 years of age.
2-4 On the other hand, studies have drawn attention to the importance of including the 40-49 year age group in screening programs, with some publications showing a reduction of up to 25% in breast cancer mortality in this age group.
5-7Delay in diagnosing and treating breast cancer results in more advanced stages at the first presentation and correlates with a reduction in survival.
8 In addition to the widely acknowledged psychological, socioeconomic and cultural barriers, a new obstacle appeared at the end of 2019, Covid-19. The spread of SARS-CoV-2 led to unprecedented disruptions in the healthcare systems.
9,10Lockdown policies, suspension of non-urgent services, and recommendations from professionals caused widespread interruption of breast cancer screening and postponement of routine consultations and elective surgeries. Although short-term delays in screening were initially considered unlikely to affect mortality, several studies subsequently reported reductions in imaging, diagnostic procedures, and oncological surgeries, particularly in low- and middle-income countries.
11,12Many countries postponed elective cancer surgeries to reallocate healthcare resources to treat patients affected by the pandemic.
13 Brazil was no exception. Despite being guided by a
Sistema Único de Saúde (SUS) (Brazilian Public Health System), the country faced shocking inequalities to access specialized cancer care, especially in the North and Northeast regions.
1 In these settings, restrictions in transportation, reallocation of hospital resources, and fear of Covid-19 worsen the pre-existing delays. Paraíba (PB), a State with significant socioeconomic vulnerability, relies heavily on a single referral center, which manages over 70% of cancer cases in SUS.
2 To understand how the pandemic affected the diagnosis and treatment in such contexts is essential to inform emergency preparedness and strengthening oncological care.
In this regard, the objective of this study was to determine changes in the diagnosis and treatment of breast cancer among women treated at a public referral hospital in Paraíba during the Covid-19 pandemic, comparing indicators from the pre-pandemic and pandemic periods.
MethodsA retrospective cohort study was conducted to describe changes in breast cancer diagnosis and treatment among women using SUS in the State of Paraíba. The site selected for the study was
Hospital Napoleão Laureano, the main cancer referral hospital in the State, responsible for assisting 2.2% of all cancer patients in Paraíba, both from the public and private network, but predominantly a public sector.
2 The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies was followed.
14The records of eligible patients were selected in accordance with the following inclusion criteria: women with the following diagnosis: ICD-10 D05.1 (intraductal carcinoma
in situ of breast / ductal carcinoma
in situ – DCIS) and/or ICD-10 C50 (malignant neoplasm of the breast, encompasses all invasive breast carcinoma, whether of ductal, lobular, or another specified site within the breast, including any stage and any histological type), who were SUS patients . The exclusion criteria consisted of incomplete or missing medical records. Records were excluded if diagnosis or treatment was incomplete or performed primarily at another institution, resulting in missing or insufficient information.
The study analyzed medical records from the period of November 2017 and October 2018 (pre-pandemic period) and between January and December 2020 (pandemic period). The year 2019 was excluded because cases were diagnosed before the pandemic, but treatments continued into the pandemic, hindering a clear distinction between the intervals analyzed.
The variables analyzed were collected from the medical records and consisted of:
biological, sociodemographic and lifestyle characteristics and comorbidities (age, weight, height, body mass index [BMI], classification of weight, skin color/ethnicity, schooling, place of residence, smoking and alcohol consumption);
reproductive characteristics (menarche, menopausal status, number of pregnancies, number of deliveries, breastfeeding, use of hormonal contraception, use of hormone therapy);
clinical characteristics (main complaint, findings in clinical examination, lesion size at clinical examination, diagnosis staging , diagnostic modality, imaging findings, histopathology findings, postoperative staging, molecular subtype and treatment modalities) and
characteristics of the care provided following the diagnosis hypothesis/ indicators of the pandemic impact (time between detection of suspicious findings in imaging exams and the beginning of treatment - and its partial time intervals, the percentage of missed appointments of patients returning later than previously scheduled, and the percentage of patients who abandoned treatment).
Descriptive and statistics included frequencies, means and standard deviations for normally distributed variables, and medians and interquartile ranges (IQR) for asymmetrical distributions. Differences between time periods were evaluated using chi-square or Fisher's exact test for categorical variables and Student's
t or Mann-Whitney tests for continuous variables, according to distribution. Relative risks (RR) and 95% confidence intervals (95%CI) were estimated. Analyses were performed by using Epi Info 3.5.4, with
p<0.05 considered statistically significant.
This study was approved by the Research Ethics Committee at the
Instituto de Medicina Integral Prof. Fernando Figueira (IMIP), Brazil (protocol no. 5.574.350/2022), in accordance with national standards and the principles of the Declaration of Helsinki. Written informed consent was obtained from the participants before data collection. When contact could not be established after multiple attempts, the requirement for informed consent was waived by the Ethics Committee, with strict adherence to national regulations regarding data confidentiality and secrecy.
ResultsA total of 218 women met the inclusion criteria, 114 in the pre-pandemic period and 104 during the pandemic (Figure 1).
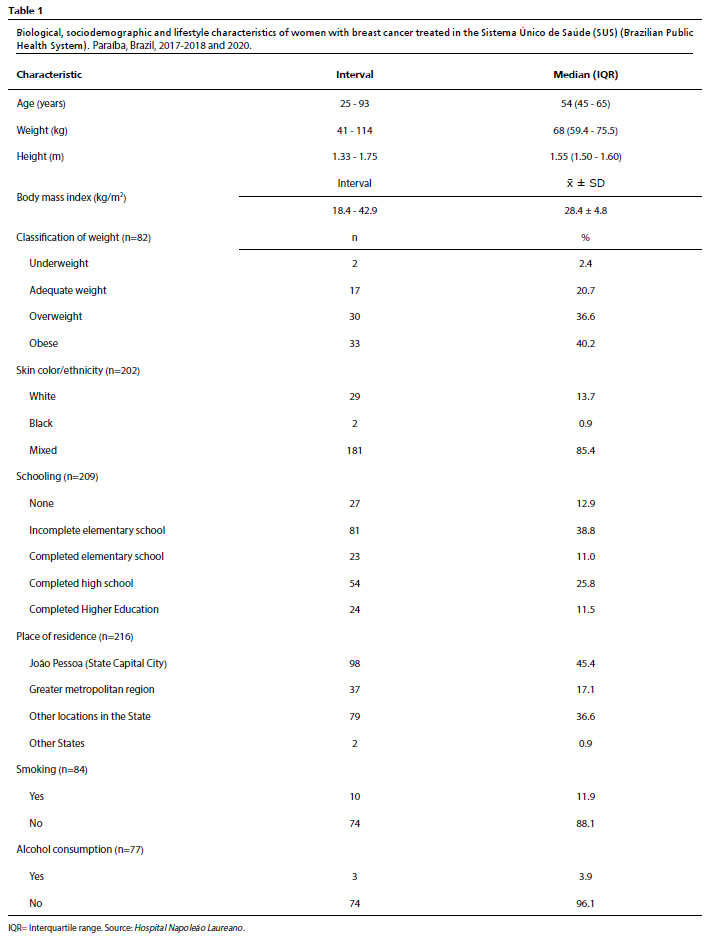
The median age was similar between the groups (54
vs. 53.5 years). Most women were mixed colored skin, overweight or obese, and had low schooling levels, with no relevant differences across periods (Table 1).
Clinical presentation was predominantly palpable breast lump, and most tumors were invasive carcinomas, mainly invasive ductal carcinoma, stage II, and luminal subtype. Surgical treatment consisted mostly of mastectomy, with immediate reconstruction performed in 24.8% of the overall cases. (data not shown in Table).
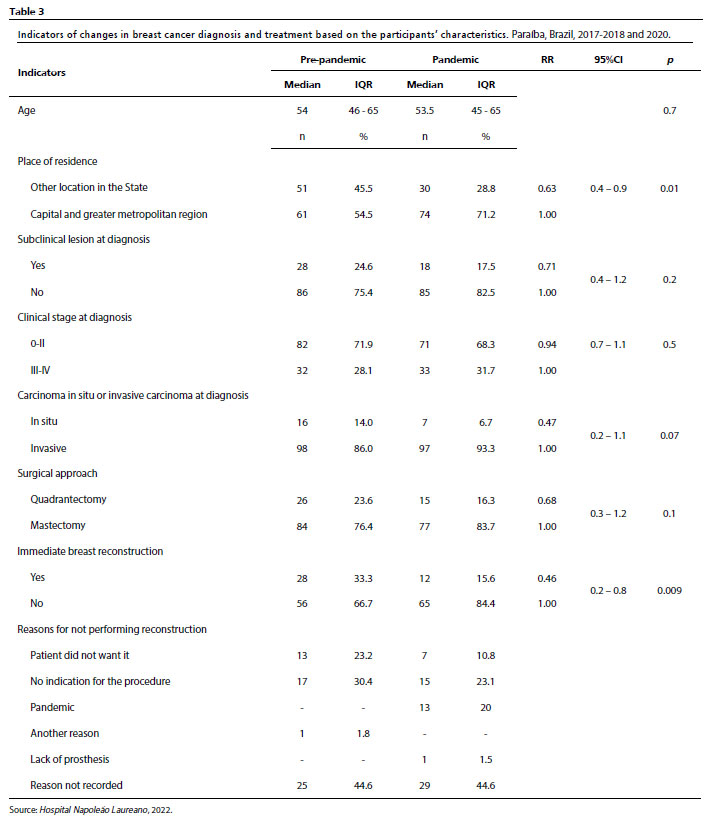
When comparing the periods, significant differences emerged in access and care. Women living outside the State capital and its metropolitan region were less likely to access the referral hospital during the pandemic (RR=0.63; 95%CI=0.4–0.9;
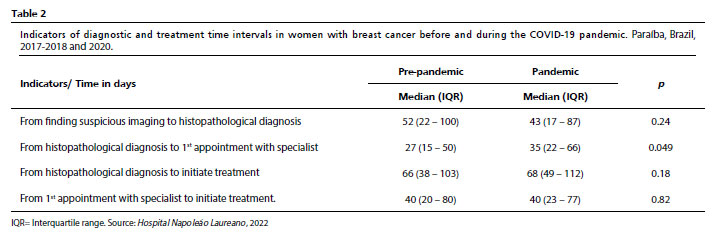
p=0.01). The interval between histopathological diagnosis and the first consultation with a specialist increased from a median of 27 days pre-pandemic to 35 days in the pandemic (
p=0.049). Other diagnostic intervals showed no significant differences (Table 2).
Although staging at diagnosis did not differ significantly between groups, immediate breast reconstruction decreased markedly during the pandemic (33.3%
vs. 15.6%; RR=0.46; 95%CI=0.2–0.8;
p=0.009) (Table 3).
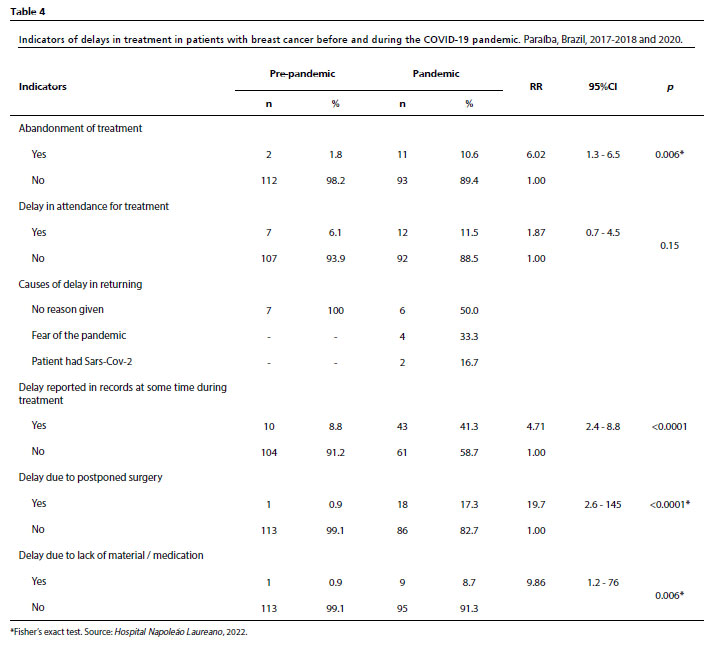
Indicators of care continuity were adversely affected. Abandonment of treatment increased from 1.8% to 10.6% during the pandemic (RR=6.02; 95%CI= 1.3–6.5;
p=0.006). The occurrence of delays recorded at any point during treatment were more frequent during the pandemic period. (8.8%
vs. 41.3%; RR=4.71; 95%CI=2.4–8.8;
p<0.0001). Postponed surgeries (0.9%
vs. 17.3%; RR=19.7;
p<0.0001) and delays due to lack of material or medication (0.9%
vs. 8.7%; RR=9.86;
p=0.006) were also significantly higher during the pandemic (Table 4).
DiscussionThis study compared the diagnosis and treatment of breast cancer before and during the Covid-19 pandemic in Paraíba and showed that the most relevant disruptions occurred in access to specialized care and in continuity of the treatment. Delays, particularly due to postponed surgeries and lack of medication, became substantially more frequent, and immediate breast reconstruction decreased markedly. Fear of Covid-19 was a frequent reason for missing appointments, and reduced attendance among women living outside the metropolitan region highlighted how travel restrictions and service concentration intensified existing barriers.
There was a marked reduction in breast cancer care during the pandemic.
15,16 A concern finding in the present study was the reduced attendance of women living outside the State capital or metropolitan region. This likely reflects on mobility barriers and the concentration of oncology services in a single referral center, which already posed challenges before the pandemic but became more pronounced with travel restrictions.
There was no significant difference in time between suspicious imaging findings and histopathological diagnosis. Although initial diagnostic intervals remained stable, meeting legally mandated deadlines continues to be challenging. Brazilian laws require diagnostic confirmation within 30 days and treatment initiation within 60 days, but delays were already common before the pandemic.
17,18 In this study, the median time from diagnosis to treatment initiation slightly exceeded 60 days in both periods, indicating that the system operated under structural strain even before COVID-19.
The pandemic intensified pre-existing vulnerabilities in the Northeast of Brazil, where services for specialist are concentrated in capitals and where socioeconomic disadvantages and long traveling distances limit access to oncological care.
19,20 These structural barriers likely contributed to abandonment of treatment and the marked reduction in immediate breast reconstruction seen in this study, a pattern also reported in European centers during periods of restricted surgical capacity.
21,22A study conducted in Brazil in 2019 to evaluate the structure of public healthcare services in the country showed that specialized care centers within SUS are few and concentrated in the capitals, resulting in insufficient coverage for the rural populations. The distance and cost of traveling aggravate these disparities.
19 According to the
Instituto Brasileiro de Geografia e Estatística (IBGE)(Brazilian Institute of Geography and Statistics), nearly half of the poverty in the country is concentrated in the Northeast.
20 This vulnerability was amplified by the pandemic at all healthcare levels.
Treatment delays were markedly more frequent during the pandemic, consistent with international evidence showing increased oncologic risk with postponed surgery. Shortages on surgical materials and hospital overload during Covid-19 waves also disrupted care. The combined effects of delays, uncertainty and fear contributed to missed appointments and heightened psychosocial distress, as reported worldwide.
23,24Abandonment of treatment increased more than sixfold during the pandemic, a pattern also described in other oncological settings during Covid-19. In this study, fear of infection and logistical restrictions were frequent reasons for missing appointments, suggesting that psychological distress acted together with structural barriers to disrupt care continuity f.
24,25This study has limitations. Its retrospective design depended on the completeness of medical records, which led to the exclusion of cases with insufficient information and limited the analysis of some clinical variables. The assessment was restricted to a single public referral center, which may not capture the full heterogeneity of breast cancer care in the State. In addition, the study periods did not allow evaluation of long-term outcomes or of the cumulative effect of screening interruptions on stage at diagnosis. Finally, it was not possible to follow women who abandoned the treatment, restricting conclusions regarding downstream clinical consequences.
The study also has strengths. It analyzed a comprehensive cohort of women assisted at SUS, using standardized data extraction across two well-defined periods. By situating the findings within a region characterized by socioeconomic vulnerability and high dependence on a single oncological center, the study provides contextually relevant insight into how Covid-19 pandemic disrupted care in settings where structural barriers were already present. The inclusion of detailed time-interval indicators adds precision to the evaluation of diagnostic and therapeutic delays.
In Conclusion, the COVID-19 pandemic exacerbated pre-existing vulnerabilities in breast cancer care in Paraíba, leading to reduced access for women living outside the metropolitan area, increased delays, greater abandonment of treatment and a substantial decline in immediate breast reconstruction. Although initial diagnostic intervals remained relatively stable, care continuity was significantly affected. These findings underscore the need for strategies that strengthen referral networks, decentralize diagnostic capacity and protect oncological services during public health emergencies, particularly in regions where access is structurally constrained.
References1. World Health Organization (WHO); Global Cancer Observatory (GLOBOCAN). All cancers, 2020. [
Internet]. [access in 2026 Jan 8]. Available from:
https://gco.iarc.who.int/media/globocan/factsheets/cancers/39-all-cancers-fact-sheet.pdf2. Instituto Nacional do Câncer José de Alencar Gomes da Silva (INCA). Recomendações do Ministério da Saúde para o rastreamento do câncer de mama [Recommendations from the Ministry of Health for breast cancer screening]. [
Internet]. [access in 2026 Jan 8]. Available from:
https://www.inca.gov.br/noticias/confira-recomendacoes-do-ministerio-da-saude-para-o-rastreamento-do-cancer-de-mama3. Canadian Task Force on Preventive Health Care (CTFPHC). Breast Cancer Update (2018) - Recommendations on screening for breast cancer in women 40-74 years of age who are not at increased risk. [
Internet]. [access in 2026 Jan 5]. Available from:
https://canadiantaskforce.ca/guidelines/published-guidelines/breast-cancer-update/4. International Agency for Research on Cancer (IARC) - Working Group. Effectiveness of Breast Cancer Screening - Breast cancer screening - NCBI Bookshelf. IARC handbooks of cancer prevention. [
Internet]. [access in 2026 Jan 16]. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK546549/5. Duffy SW, Vulkan D, Cuckle H, Parmar D, Sheikh S, Smith RA,
et al. Effect of mammographic screening from age 40 years on breast cancer mortality (UK Age trial): final results of a randomised, controlled trial. Lancet Oncol. 2020; 21 (9): 1165-72.
6. Mao Z, Nyström L, Jonsson H. Breast cancer screening with mammography in women aged 40-49 years: impact of length of screening interval on effectiveness of the program. J Med Screen. 2021; 28 (2): 200-6.
7. Hendrick RE, Baker JA, Helvie MA. Breast cancer deaths averted over 3 decades. Cancer. 2019; 125 (9):1482-8.
8. Zielonke N, Gini A, Jansen EEL, Anttila A, Segnan N, Ponti A,
et al. Evidence for reducing cancer-specific mortality due to screening for breast cancer in Europe: A systematic review. Eur J Cancer. 2020; 127:191-206.
9. Oliveira WK, Duarte E, França GVA, Garcia LP. Como o Brasil pode deter a COVID-19 [How Brazil can hold back COVID-19]. Epidemiol Serv Saúde. 2020; 29 (2): e2020044.
10. World Health Organization (WHO). Timeline of WHO's response to COVID-19. [
Internet]. [access in 2026 Jan 6]. Available from:
https://www.who.int/emergencies/diseases/novel-coronavirus-2019/interactive-timeline#event-1311. American Society of Breast Surgeons (ASBrS); American College of Radiology (ACR). ASBrS and ACR joint statement on breast screening exams during the COVID-19 Pandemic. Columbia, MD: ASBrS; 2020. [
Internet]. [access in 2025 Sep 29]. Available from:
https://www.breastsurgeons.org/docs/news/2020-03-26-ASBrS-ACR-Joint-Statement.pdf12. European Society for Medical Oncology (ESMO). Cancer care during the COVID-19 pandemic. [access in 2025 Aug 9]. Available from:
https://www.esmo.org/for-patients/patient-guides/cancer-care-during-the-covid-19-pandemic13. Hanna TP, King WD, Thibodeau S, Jalink M, Paulin GA, Harvey-Jones E,
et al. Mortality due to cancer treatment delay: systematic review and meta-analysis. BMJ. 2020; 371: m4087.
14. STROBE Initiative. STROBE Statement—checklist of items for reports of observational studies. 2007. [
Internet]. [access in 2025 Nov 24]. Available from:
https://www.strobe-statement.org/checklists/15. Nascimento JHF, Silva CN, Gusmão-Cunha A, Neto MMS, Andrade AB. Effects of the COVID-19 pandemic on delays in diagnosis-to-treatment initiation for breast cancer in Brazil: a nationwide study. Ecancermedicalscience. 2023; 17: 1570.
16. Duarte MBO, Argenton JLP, Carvalheira JBC. Impact of COVID-19 in cervical and breast cancer screening and systemic treatment in São Paulo, Brazil: an interrupted time series analysis. JCO Glob Oncol. 2022; (8): e2100371.
17. Brasil. Lei nº 13.896, de 30 de outubro de 2019. Altera a Lei nº 12.732/2012 para que os exames relacionados ao diagnóstico de neoplasia maligna sejam realizados no prazo de 30 (trinta) dias, no caso em que especifica. Brasília (DF): DOU de 31 de outubro de 2019. [
Internet]. [access in 2025 May 30]. Available from:
https://www.planalto.gov.br/ccivil_03/_ato2019-2022/2019/lei/l13896.htm18. Brasil. Lei nº 12.732, de 22 de novembro de 2012. Dispõe sobre o primeiro tratamento de paciente com neoplasia maligna comprovada e estabelece prazo para seu início. Brasília (DF): DOU de 23 de novembro 2012. [
Internet]. [access in 2025 May 30]. Available from:
https://www.planalto.gov.br/ccivil_03/_ato2011-2014/2012/lei/l12732.htm19. Hospital Napoleão Laureano. Nossos números - Hospital Napoleão Laureano. [Our numbers - Napoleão Laureano Hospital]. [
Internet]. [access in 2025 May 30]. Available from:
http://hlaureano.org.br/quem-somos/nossos-numeros20. Belandi C. Síntese de Indicadores Sociais - Em 2021, pobreza tem aumento recorde e atinge 62,5 milhões de pessoas, maior nível desde 2012 [Summary of Social Indicators - In 2021, poverty has a record increase and reached 62.5 million people, the highest level since 2012]. Agência IBGE Notícias; 2022. [
Internet]. [access in 2025 Aug 24]. Available from:
https://agenciadenoticias.ibge.gov.br/agencia-noticias/2012-agencia-de-noticias/noticias/35687-em-2021-pobreza-tem-aumento-recorde-e-atinge-62-5-milhoes-de-pessoas-maior-nivel-desde-201221. Toss A, Isca C, Venturelli M, Nasso C, Ficarra G, Bellelli V,
et al. Two-month stop in mammographic screening significantly impacts on breast cancer stage at diagnosis and upfront treatment in the COVID era. ESMO Open. 2021; 6 (2): 100055.
22. Sgarzani R, Macrì G, Gurrado A, Curcio A, De Lorenzi F, Galimberti V,
et al. The impact of COVID-19 pandemic on breast surgery in Italy: a multi-centric retrospective observational study. Updates Surg. 2023; 75 (3): 735-41.
23. Myers C, Bennett K, Kelly C, Walshe J, O'Sullivan N, Quinn M,
et al. Impact of COVID-19 on health care and quality of life in women with breast cancer. JNCI Cancer Spectr. 2023; 7 (3): pkad033.
24. Vanni G, Materazzo M, Pellicciaro M, Ingallinella S, Rho M, Santori F,
et al. Breast cancer and COVID-19: the effect of fear on patients' decision-making process. In Vivo. 2020; 34 (3 Suppl.): 1651-9.
25. Massicotte V, Ivers H, Savard J. COVID-19 pandemic stressors and psychological symptoms in breast cancer patients. Curr Oncol. 2021; 28 (1): 294-300.
Authors' contributionRamalho TC: conceptualization, data curation, investigation, formal analysis, writing—original draft.
Katz L: conceptualization, methodology, supervision, writing—review and editing.
Ramalho IC: data curation, investigation, validation, writing—review and editing.
Carneiro da Cunha ACM: research, visualization, writing – review and editing.
Amorim MMR: conceptualization, methodology, project management, supervision, writing – review and editing.
All authors approved the final version of the article and declare no conflict of the interest.
Data availabilityAll datasets supporting the result of this study are included in the article.
Received on June 15, 2025
Final version presented on November 28, 2025
Approved on December 30, 2025
Associated Editor: Alex Sandro Souza


 ; Leila Katz1
; Leila Katz1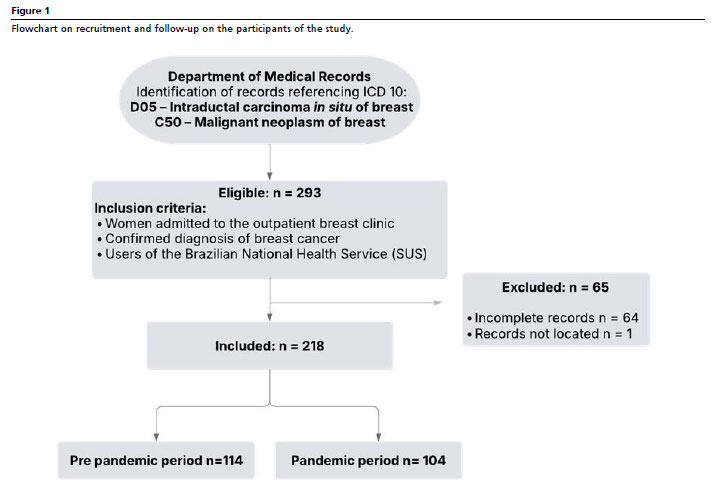






 Ler em português
Ler em português