ABSTRACT
OBJECTIVES: to evaluate pregnant women's knowledge on oral health and its association with sociodemographic characteristics.
METHODS: this exploratory cross-sectional study included a convenience sample of 69 women attended at a prenatal referral outpatient clinic in a Brazilian city. Data were collected using an oral health questionnaire adapted from Bianco (2010); higher scores indicated better knowledge. The outcome "knowledge on oral health " was dichotomized at the sample mean (less/more). Sociodemographic and oral health-related variables were obtained from the questionnaire, and associations were tested using Pearson's chi-square/Fisher's exact tests (α=0.05).
RESULTS: most participants who were unemployed, had completed secondary education, and had low family income; 50.7% had less knowledge on oral health. Lower scores involved primary and permanent dentition, tooth eruption and exfoliation, and causes of dental caries, halitosis, and oral cancer. In bivariate analyses, women with lower family income and lower schooling were more frequently classified as having lower knowledge on oral health, whereas employed women were more frequently classified as having higher knowledge.
CONCLUSION: pregnant women showed limited knowledge on oral health, especially among those in socioeconomically more vulnerable groups. Given the cross-sectional design and the use of an unvalidated instrument for pregnant women, findings should be interpreted cautiously and may inform educational strategies in similar services.
Keywords:
Oral health, Pregnant women, Knowledge, Cross-sectional study, Observational study
IntroductionPediatric Dentistry (AAPD) guidelines recommend that health and dental routines begin by one year of age.
1Although transient cognitive difficulties may occur, health education during childhood is foundational, helping these habits continue onto adulthood.
2,3 In this context, limited maternal knowledge regarding oral health may contribute to oral problems in children. Understanding why some mothers neglect their own oral health consequently, their children's, is therefore important.
4,5 This concern is particularly relevant given the availability of oral health promotion programs for pregnant women, including verbal counseling, health education, and promotional interventions.
5–7Mothers with greater access to information are more likely to intervene positively in their children's health.
8Health behavior encompasses a complex set of attitudes, knowledge, and practices that influence oral health.
3 A quasi-experimental study reported that prevention and health-promotion messages sent by health agents to pregnant women encouraged the use of the health system for more in-depth assessment and improved knowledge about maternal and newborn care
9. Multidisciplinary work is essential for oral health
2; the sharing of skills between health professionals can bring benefits across disciplines, and community-based multidisciplinary teams can play an essential and complementary role in promoting oral health and expanding pathways to prevent oral disease.
2Oral health knowledge refers to the specific information individuals hold about the causes, consequences, and prevention of oral diseases, such as understanding the role of dental biofilm, sugar intake, primary dentition, and the timing of the first dental visit. Oral health literacy is a broader construct that encompasses the cognitive and social skills that determine the motivation and ability to access, understand, evaluate, and use health information in everyday decisions. Although these dimensions are closely related, but not identical; measuring knowledge through correct answers in a structured questionnaire captures only one component of oral health literacy. Recent Brazilian studies with pregnant women have shown that lower oral health literacy is associated with poorer oral health–related quality of life and a higher prevalence of untreated dental caries, highlighting the influence of social determinants on how information is accessed and used.
10,11 In this study, we focus specifically on the dimension of knowledge, operationalized by the score obtained using a questionnaire on primary dentition, dental caries, and preventive practices. Throughout this manuscript, we use the term "knowledge on oral health" to describe the measured outcome, and we mention "oral health literacy" only when referring to the broader construct.
We have identified a gap in evidence regarding pregnant women's knowledge on oral health, including primary and permanent dentition, risk factors for cavities, halitosis, and oral cancer, preventive practices, and dental treatment during pregnancy. Therefore, this study aimed to evaluate pregnant women's knowledge on oral health and to investigate its association with sociodemographic characteristics. Based on a social determinant of health framework, we hypothesized that women in more vulnerable socioeconomic positions (lower schooling, lower family income, and being a homemaker) would be more likely to present lower knowledge on oral health than those with more favorable socioeconomic conditions.
MethodsThis study is part of a broader research project on oral health and maternal care, approved by the Research Ethics Committee of IMED (Passo Fundo, RS, Brazil) under opinion number 689.475 and CAAE 31581214.8.0000.5319, issued on October 29, 2014. The 2022 data collection was conducted under the same ethical protocol, which remains valid as part of this larger project. All procedures adhered to the guidelines of the National Health Council Resolution 466/2012, ensuring confidentiality, anonymity, and voluntary participation by all the participants in signing an Informed Consent Form (ICF) before completing the questionnaire. This work was written according to the requirements of STROBE.
12This exploratory cross-sectional study was conducted at the prenatal outpatient clinic of a municipal public hospital. This clinic is a public reference service for prenatal care, especially for medium- and high-risk pregnancies, but it is not the only point of care for pregnant women in the city, as low-risk pregnancies may also be followed in primary health care units. For operational reasons, recruitment was restricted to this reference outpatient clinic, which should therefore be understood as a convenience sample of women who attended this service during the data-collection period. The hospital is in the city of Passo Fundo, in the State of Rio Grande do Sul, South of Brazil. The city has a land area of approximately 784.4 km
2 and an estimated population of 206,215 inhabitants, according to the
Instituto Brasileiro de Geografia e Estatistica (IBGE)
13 data. (Brazilian Institute of Geography and Statistics Passo Fundo is a regional health referral center that provides specialized maternal and child health care services, including prenatal, dental, and educational programs within the
Sistema Único de Saúde (SUS) (Brazilian Public Health System).
We adopted a convenience sampling of all pregnant women treated at the outpatient clinic during the data collection period (July–September 2022), with no restriction by gestational age and according to the eligibility criteria (able to read and answer the questionnaire). The n 69 corresponded to the total number of participants included at the end of the collection period, reflecting the service demand during this interval. No prior sample size calculation was performed, since the main objective was to describe the level of knowledge on oral health and to explore bivariate associations with sociodemographic characteristics in a context representative of the service routine. Although no priori calculation was performed, this sample size yields an estimated margin of error of approximately 12 percentage points for the main proportions, which is acceptable for an exploratory cross-sectional study. As this was a convenience sample from a single prenatal service, it is not representative of all pregnant women in the city nor of the
Sistema Único de Saúde (SUS) (Brazilian Public Health System) as a whole; therefore, findings should be interpreted as exploratory.
Data were collected from July to September 2022 using a self-administered questionnaire for pregnant women who attended the outpatient clinic by a single researcher in the waiting room of the site, while the pregnant women were waiting for medical care and addressed questions about oral health. It includes primary and permanent dentition, oral hygiene habits, prevention and treatment of some oral diseases, and sociodemographic characteristics of pregnant women. As inclusion criteria, all pregnant women were invited to complete the questionnaire regardless of their trimester of pregnancy. The instrument used was the oral health questionnaire developed by Bianco,
14 originally applied to community health workers and users of the
Sistema Único de Saúde (SUS) (Brazilian Public Health System). For this study, the questionnaire was adapted for pregnant women through language revision and term adjustments by the research team and pre-tested with five pregnant women from the same outpatient clinic to assess comprehension and response time. No formal analyses of internal consistency (Cronbach's alpha), construct validity, or stability (test–retest) were performed, as the instrument was used in an exploratory and descriptive manner within the context of prenatal care. The complete questionnaire is available in the Appendix of this manuscript.
All questionnaires were reviewed at the time of the collection to verify completeness. Missing responses were rare (<5%) and not concentrated in any specific variable. Therefore, analyses were conducted using complete-case analysis, with no imputation of missing data.
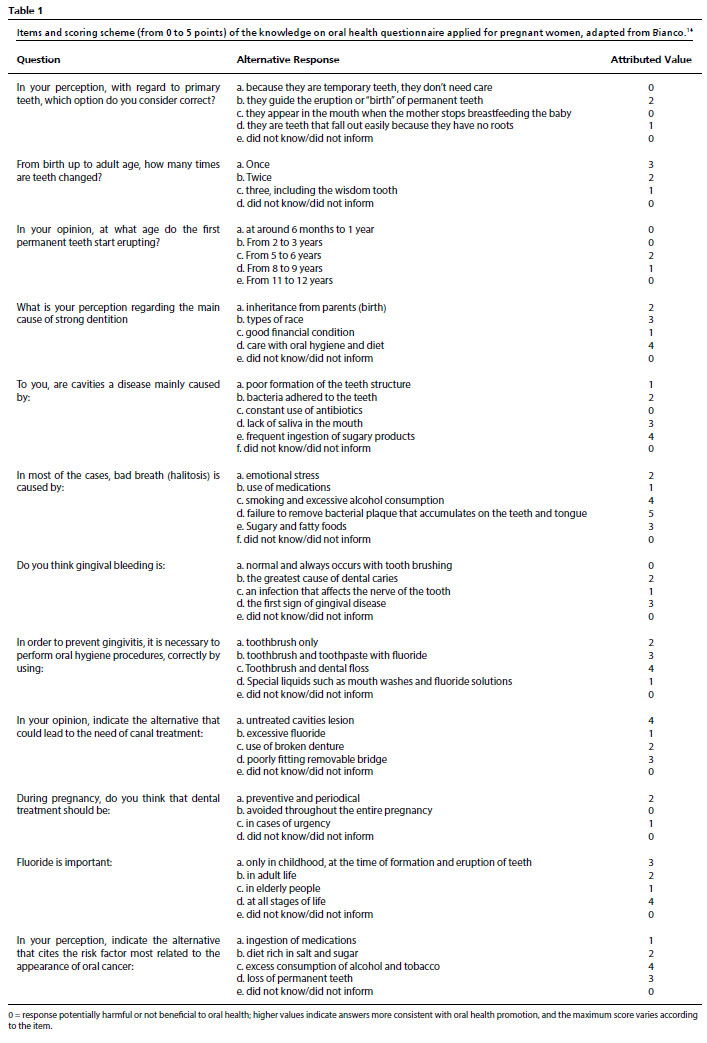
The values assigned to each response are different, using the principles of beneficence and non-maleficence as criteria. According to Bianco,
14 responses that may lead to behaviors that do not improve a person's oral health status are considered to have a value of zero (0), or if these responses indicate that the individual may use their knowledge to adopt procedures that may in some way harm their oral health status. The higher the final score, the more relevant the knowledge of the pregnant woman. The detailed scoring scheme for each item and response option (ranging from 0 to 5 points, depending on the item) is presented in Table 1, adapted from Bianco.
14 The dependent variable "knowledge on oral health" was initially analyzed as a continuous score, calculated as the sum of all responses for each participant (ranging from 0 to 41 points). Measures of central tendency and dispersion were obtained (mean, standard deviation, median, and interquartile range), and the score distribution was examined to assess data symmetry and variability. For comparative and interpretative purposes, the score was also dichotomized based on the sample mean, defining "less knowledge" (17-32 ≤ mean) and "more knowledge" (33-41 > mean). This strategy has been adopted in a study using similar questionnaires applied to adult populations
14, ensuring methodological consistency with the literature and facilitating group comparison in bivariate analyses. This dichotomization is a pragmatic analytical strategy and should not be interpreted as a normative or clinical threshold of adequate knowledge.
The explanatory variables of the study were grouped into two blocks. The sociodemographic block included age group, place of residence, self-reported skin color, marital status, schooling, family income, occupation/profession, trimester of pregnancy, and having other children. The oral health–related block comprised smoking status, alcohol consumption, time of last dental visit, type of dental service usually used, having a regular dentist, use of dental services during pregnancy, frequency of tooth brushing, flossing, tongue brushing, self-perceived oral health, and history of toothache during pregnancy. All information was obtained through closed-ended questions in the same structured questionnaire applied to assess knowledge on oral health. For the analyses, these variables were categorized according to their empirical frequency distribution and in line with previous studies on social determinants of oral health, and the categories used for each variable are shown in Tables 2 and 4.
The selection of explanatory variables was guided by a theoretical model grounded in the social determinants of health framework. In this perspective, socioeconomic position (especially schooling, family income and occupation) conditions access to health information, preventive resources, and dental services, which may, in turn, influence how pregnant women acquire and consolidate knowledge on oral health during prenatal care. This conceptual model supported the inclusion of sociodemographic and oral health–related variables in the bivariate analysis with the knowledge outcome.
Data were analyzed using IBM SPSS Statistics version 20.0. Descriptive statistics were used to summarize all variables, with absolute and relative frequencies for categorical variables and measures of central tendency and dispersion for the knowledge on oral health score. To judge whether each question was difficult to answer, we used a cut-off point of 70% agreement with the correct answer. That is, if 70% or more of the answers were correct, it was judged that pregnant women had more knowledge about the topic in question.
Associations between knowledge on oral health (less/more) and sociodemographic characteristics were tested using Pearson's chi-square test. When the expected frequency in any cell of the contingency tables was <5, Fisher's exact test or when expected cell counts were <5 (for example, for smoking and other low-frequency categories). The significance level was set at 5% (two-sided). Given the modest sample size and the descriptive, exploratory nature of this study, we did not estimate prevalence ratios (PR) or fit multivariable regression models; the analysis was intentionally restricted to crude bivariate associations between knowledge on oral health and the explanatory variables, and this analytical decision is acknowledged as a limitation in the Discussion.
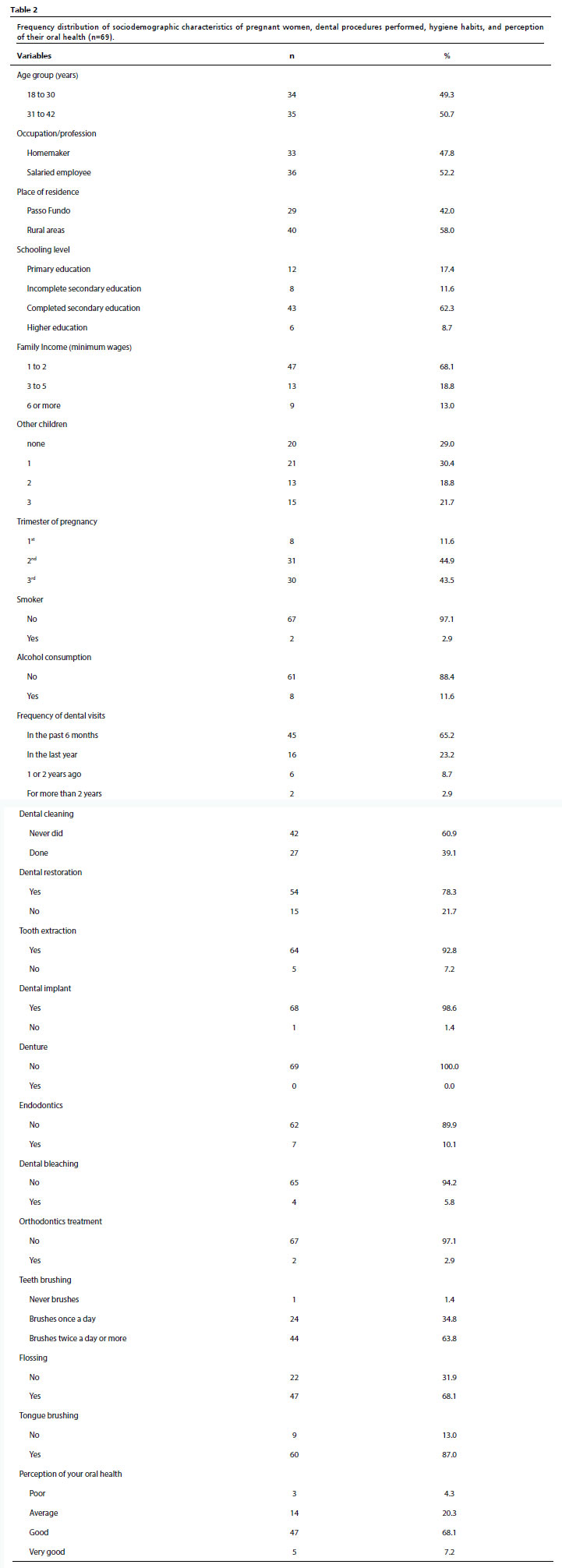
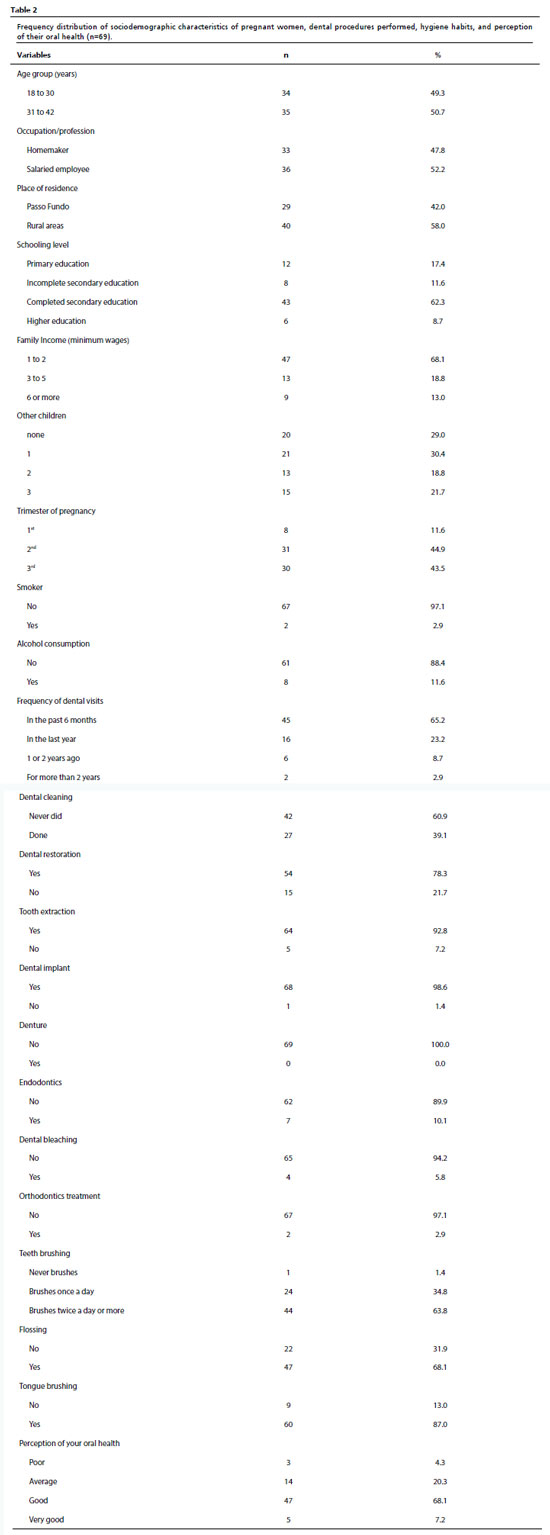
ResultsTable 2 presents the results of the frequencies of pregnant women and their distribution according to age group, occupation/profession, place of residence, schooling, family income, other children, trimester of pregnancy, smoking, alcohol consumption, last dental visit, dental procedures already performed, hygiene habits such as tooth brushing, tongue brushing, use of dental floss, and perception of their own oral health. The pregnant women's mean age was 30.45 (SD 6.13) years. Almost half of the pregnant women were unemployed (47.8%), lived in rural areas (58%), had completed secondary education (62.3%), and had a family income of 1 to 2 minimum wages (68.1%).
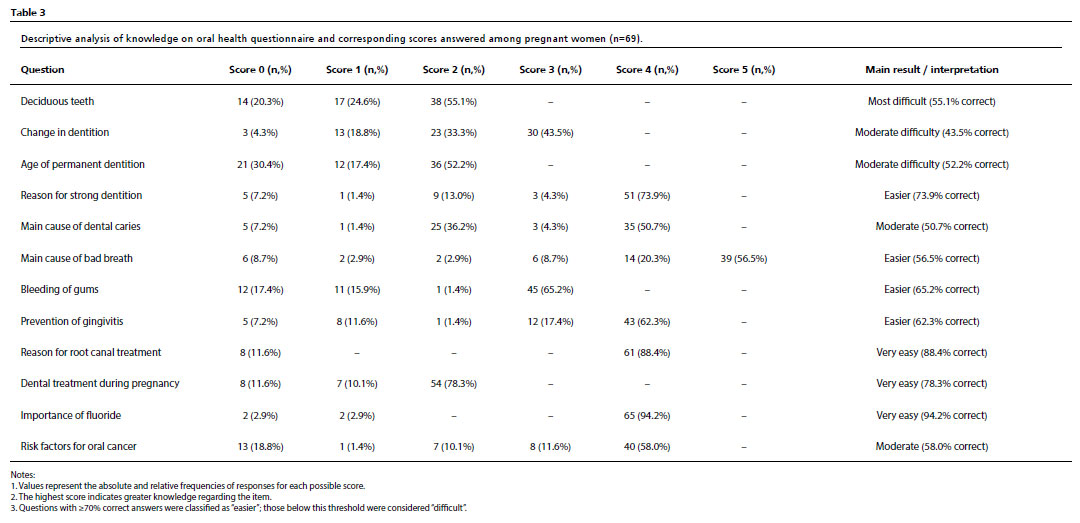
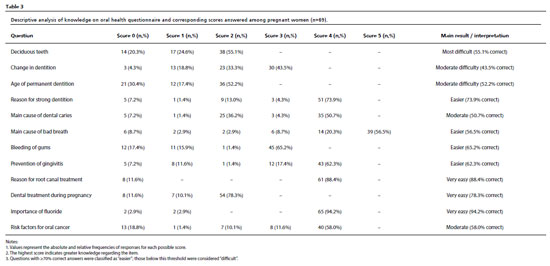
Table 3 shows the absolute and relative frequencies of the responses to each item of the questionnaire on oral health knowledge. When the total score was dichotomized at the sample mean, 50.7% of the pregnant women were classified as having less knowledge on oral health and 49.3% as having more. Overall, only some questions reached more than 70% of the correct answers, indicating that knowledge was suboptimal in this sample. The items with the greatest difficulty were those related to tooth eruption and exfoliation, with only 43.5% correct responses, the birth of the first permanent teeth (52.2%), and baby teeth (55.1%). In addition, questions about oral diseases as the main cause of tooth decay (50.7%), bad breath (56.5%) and risk factor for oral cancer (58%) also had relatively low proportions of correct answers. The questions with the most correct answers were the importance of using fluoride (94.2%), the need for endodontic treatment (88.4%), and the main factor for strong teeth (73.9%). All response frequencies (correct and incorrect answers) are shown in Table 3 as absolute and relative values (n and %), to ensure transparency and reproducibility of the findings.
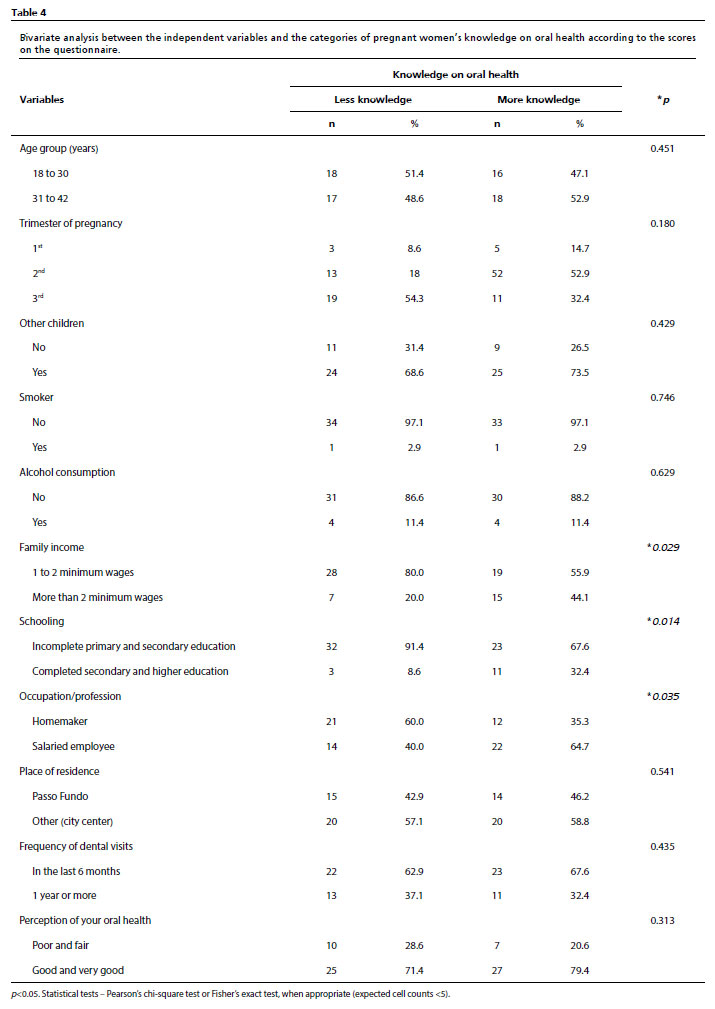
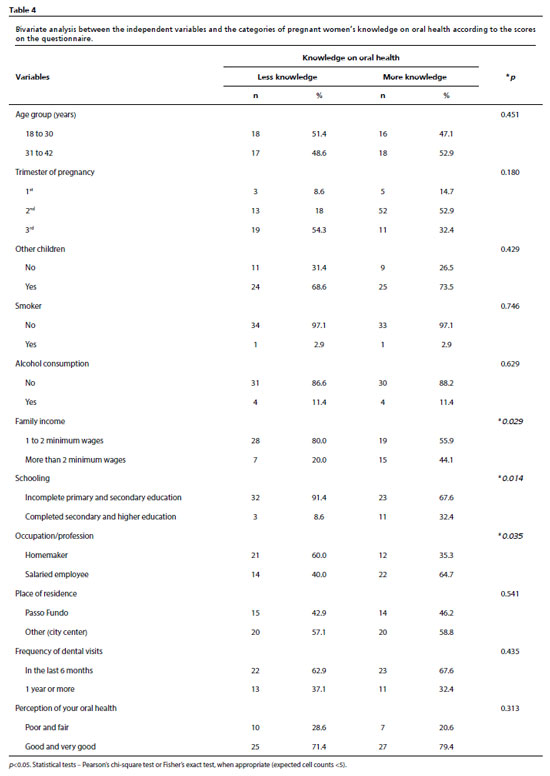
The following variables were tested with " knowledge on oral health " in the bivariate analysis using Pearson's chi-squared test: "age group", "trimester of pregnancy", "having other children", "being a smoker", "consume alcohol", "family income", "occupation/profession", "schooling", "dental visit", "city of residence" and "oral health perception". When the expected frequency in any cell of the contingency tables was <5, Fisher's exact test was applied instead of the chi-square test. Among the associations tested, statistically significant bivariate differences (
p<0.05) were observed only for socioeconomic variables. Participants with lower family income (80%) and lower schooling (91.4%) were more frequently classified as having lower knowledge on oral health, whereas employed pregnant women were more frequently classified as having higher knowledge (64.7%) (Table 4).
DiscussionThis exploratory cross-sectional study showed that approximately half of the pregnant women receiving care in a public prenatal clinic were classified as having lower knowledge on oral health according to a structured questionnaire. Lower schooling, lower family income and being a homemaker were associated with less knowledge, indicating a clear social gradient in the distribution of oral health information among pregnant women in this context. Even in a setting where prenatal care is offered free of charge, women in more vulnerable socioeconomic positions appear to have fewer opportunities to access, understand, and internalize key messages about oral disease prevention and the mother–child dyad's oral health.
These findings are consistent with national and international evidence showing that social determinants are associated with oral health literacy and oral health outcomes during pregnancy. Recent Brazilian studies have reported that pregnant women with lower oral health literacy present worse oral health–related quality of life and a higher prevalence of untreated dental caries.
10,11 In line with this literature, the dimension of knowledge assessed in our study can be interpreted as one component of the broader construct of oral health literacy, which seems particularly sensitive to educational, economic, and occupational inequalities. Women with more years of schooling and higher income may have greater exposure to written and digital health information, more positive experiences with dental services, and better conditions to transform information received during prenatal care into concrete preventive behaviors. Accordingly, we refer to our outcome as "knowledge on oral health" (dimension of knowledge), avoiding interchangeable use with "oral health literacy".
From a public health perspective, the results reinforce the need to incorporate structured oral health education into prenatal care, prioritizing women in socially vulnerable situations. Integrating dentists into prenatal teams, offering educational group sessions, and providing culturally appropriate educational materials which may help reduce inequalities in the knowledge on oral health and, indirectly, in maternal and child oral health outcomes. At the same time, our findings should be interpreted with caution. The use of convenience sampling from a single reference service may have introduced selection bias and limited the generalizability of the results. The questionnaire used was originally developed for another population and has not undergone formal psychometric validation for pregnant women, which may reduce the accuracy of the score and the adequacy of some options of response. Data were self-reported and are therefore susceptible to recall and social desirability biases, especially regarding oral hygiene practices and the use of dental service. Psychosocial factors such as social support or social capital, which may influence how information circulates among pregnant women, were not assessed. Finally, the analysis relied exclusively on crude bivariate associations, without estimating effect measures such as prevalence ratios or adjusting for potential confounders; future studies with larger and more diverse samples should validate specific instruments to pregnant women and adopt multivariable models capable of clarifying the distinct contribution of social determinant to knowledge on oral health (i.e., the dimension of knowledge on oral health literacy).
In general, we found that pregnant women's knowledge on oral health was unsatisfactory, as most of the questions had a low number of correct answers. Considering that some issues are extremely important for the longevity and permanence of teeth in the mouth, both for pregnant women and their future children, these results are of great concern. Confirming our results, in a survey of pregnant women in the Republic of Croatia, the authors observed unsatisfactory knowledge among pregnant women and a lack of awareness of the importance of oral health during pregnancy and childhood.
15 There were fewer responses to questions about knowledge on oral health related to primary teeth, tooth eruption and exfoliation, and the arrival of the first permanent teeth. These specific problems are highlighted by Frazão and Marques
16 in a survey of women and community health workers, where the question related to the age at which the first permanent teeth appeared, the women had difficulty choosing the correct age (between 5 and 6 years) and many did not consider primary teeth to be essential for the eruption of permanent teeth.
The pregnant women in our study also had difficulty answering questions about the causes of tooth decay, bad breath, and risk factors for oral cancer. These are questions that indicate a high prevalence of oral problems other than oral cancer. Lakshmi
et al.
17 also reported that a large proportion of pregnant women were unaware of the role of fluoride and of gingival bleeding as a sign of disease. The questions on knowledge in this study that received the most correct answers from pregnant women were those related to the importance of using fluoride, the need for endodontic treatment, and the most important factor for strong teeth. These are topics also highlighted by Frazão and Marques,
16 in which the population interviewed considered fluoride important for oral health.
The socio-demographic profile showed that most of the pregnant women had an average age of 30 years, unemployed, lived in rural areas, had completed high school, and their family income was 1 to 2 minimum wages, had other children, and were in the second or third trimester of pregnancy at the time of the interview. This profile is similar to that reported in a study on the pregnant women's age group and educational level, whose authors report that the higher a person's schooling is, the greater their autonomy and ability to make healthy choices.
18Most of the pregnant women in the study reported having good oral hygiene habits, brushing their teeth two or more times a day, using dental floss, and brushing their tongue. This is different from the findings highlighted in a survey on the use of toothbrush and maternal brushing methods, which were considered inefficient by the authors.
19 Regarding the time of the last dental visit, more than 50% of pregnant women in this study visited the dentist in the last 6 months, mainly for prophylaxis and restorative procedures. This contrasts with research by Adeniyi
et al.
20 who found that few of the mothers interviewed visited the dentist during pregnancy and considered it a barrier to access oral health, probably for financial reasons.
In terms of perceptions of their oral health, most are satisfied, reporting good and excellent oral health. This is in line with the research in which 60.8% of the pregnant women surveyed considered their oral health to be good.
21 Kabali and Mumghamba
22 found that most of the pregnant women in the study had their teeth cleaned, and 95.6% of them brushed their teeth twice a day. A few of the participants had periodontal complications, and they identified themselves as having good oral hygiene habits. A few of the pregnant women in this study reported consuming alcohol and smoking during pregnancy, similar to Young-Wolff
et al.,
23 research in which alcohol use among women during prenatal care decreased from 11.6% to 8.8% and nicotine use decreased from 4.3% to 2%. Thus, during pregnancy, women tend to reduce some bad habits, which is probably for the benefit of the fetus.
When analyzing socio-demographic variables and knowledge on oral health, a statistically significant association was observed between socioeconomic variables, income, schooling, occupation of pregnant women, and knowledge level. The results were similar to those of Arora
et al.,
4 who reported an association between cultural factors and social class and lower knowledge of oral health practices. In a study by Petrauskienė
et al.
3 most mothers with less schooling and who brushed their teeth less than twice a day did not practice oral hygiene as recommended for their children. Llena
et al.
24 stated that educational level, self-care, and knowledge about oral health prevention are factors that directly interfere with the level of general knowledge about oral health among pregnant women.
This study presents some limitations that should be considered when interpreting the findings. The small sample size (n=69) and the cross-sectional, descriptive design limited the statistical power and the use of multivariate models to control confounding variables. Therefore, the associations between knowledge on oral health and sociodemographic characteristics were assessed only through bivariate analyses. Although the chi-square test identified statistically significant differences between groups, these are crude bivariate comparisons; therefore, the observed differences should not be interpreted as evidence of causal relationships, and potential confounding was not controlled. Another important limitation concerns the data collection instrument, which, although based on a questionnaire previously validated for adults,
14 was not formally psychometrically validated for pregnant women. The instrument was adapted through language revision and pre-testing with pregnant women from the same clinic, but internal consistency, construct validity, and test–retest reliability were not assessed. Therefore, there are restrictions regarding the validity and reproducibility of the scores.
In addition, the use of convenience sampling in a single prenatal reference clinic, while prenatal care in the city is also delivered in primary health care units, which may have introduced selected bias and limited the external validity of the findings. The women included in this study may differ from other pregnant women in the city about clinical risk, patterns of service use, and sociodemographic characteristics; therefore, the results should not be generalized to all pregnant women. Nevertheless, the findings faithfully represent the reality of a prenatal reference outpatient clinic within the
Sistema Único de Saúde (SUS) (Brazilian Public Health System) and provide valuable insights for planning oral health education strategies aimed at pregnant women. Finally, the sample size and the absence of multivariate adjustment represent quantitative limitations. Future studies with larger samples and analytical designs are recommended to explore more accurately the factors associated with knowledge on oral health during pregnancy.
In this exploratory cross-sectional study based on a convenience sample from a prenatal reference outpatient clinic, pregnant women showed important gaps in knowledge on oral health, particularly regarding primary/permanent dentition, cavities etiology, halitosis, and risk factors on oral cancer. In crude bivariate comparisons, lower knowledge scores were observed among women in more vulnerable socioeconomic positions. These context-specific findings are hypothesis-generating and do not allow causal inferences; they may inform the planning of oral health education actions integrated into prenatal care in similar services.
References1. Brecher EA, Lewis CW. Infant Oral Health. Pediatr Clin North Am. 2018 Oct; 65 (5): 909-21.
2. Lang AY, Carpenter LM, Silva AM, Kearney SL, Hegde S. Health promotion competencies for promoting child-oral health: Victorian multidisciplinary workforce perspectives. Health Promot J Austr. 2021 Oct; 32 (Suppl. 2): 126-38.
3. Petrauskienė S, Narbutaitė J, Petrauskienė A, Virtanen JI. Oral health behaviour, attitude towards, and knowledge of dental caries among mothers of 0- to 3-year-old children living in Kaunas, Lithuania. Clin Exp Dent Res. 2020 Apr; 6 (2): 215-24.
4. Arora A, Lucas D, To M, Chimoriya R, Bhole S, Tadakamadla SK,
et al. How Do Mothers Living in Socially Deprived Communities Perceive Oral Health of Young Children? A Qualitative Study. Int J Environ Res Public Health. 2021 Mar; 18 (7): 3521.
5. Nourijelyani K, Yekaninejad MS, Eshraghian MR, Mohammad K, Rahimi Foroushani A, Pakpour A. The influence of mothers' lifestyle and health behavior on their children: an exploration for oral health. Iran Red Crescent Med J. 2014 Feb; 16 (2): e16051.
6. Menegaz AM, Silva AER, Cascaes AM. Educational interventions in health services and oral health: systematic review. Rev Saúde Pública. 2018; 52: 52.
7. Ghaffari M, Rakhshanderou S, Ramezankhani A, Noroozi M, Armoon B. Oral Health Education and Promotion Programmes: Meta-Analysis of 17-Year Intervention. Int J Dent Hyg. 2018 Feb; 16 (1): 59-67.
8. Rocha JS, Arima L, Chibinski AC, Werneck RI, Moysés SJ, Baldani MH. Barriers and facilitators to dental care during pregnancy: a systematic review and meta-synthesis of qualitative studies. Cad Saúde Pública. 2018 Sep 6; 34 (8): e00130817.
9. Adam MB, Dillmann M, Chen MK, Mbugua S, Ndung'u J, Mumbi P, et al. Improving maternal and newborn health: effectiveness of a community health worker program in rural Kenya. PLoS One. 2014 Aug; 9 (8): e104027.
10. Araujo G, Rauber ED, Segatto MC, Pacheco SC, Knorst JK, Emmanuelli B. Oral health literacy and its association with oral health-related quality of life amongst pregnant women: a cross-sectional study. Qual Life Res. 2024; 33(1): 219-27.
11. Araujo G, Scheuermann MZ, Knorst JK, Ardenghi TM, Emmanuelli B. The Moderating Effect of Oral Health Literacy on the Relationship between Socioeconomic Conditions and Untreated Dental Caries in Pregnant Women. Caries Res. 2025 May 21: 1-9.
12. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ. 2007; 335: 806-8.
13. Instituto Brasileiro de Geografia e Estatística (IBGE). Cidades e Estados. Passo Fundo. [access 2022 Jan 22]. Available in:
https://ibge.gov.br/cidades-e-estados/rs/passo-fundo.html14. Bianco LC. Avaliação de conhecimentos em saúde bucal de agentes comunitários de saúde (ACS) e usuários do SUS de Porto Velho. [dissertação]. Taubaté (São Paulo): Universidade de Taubaté; 2010.
15. Gavic L, Maretic A, Putica S, Tadin A. Attitudes and knowledge of pregnant women about oral health. J Educ Health Promot. 2022 Feb; 11: 77.
16. Frazão P, Marques D. Influence of community health agents on the perception of women and mothers about oral health knowledge. Ciênc Saúde Coletiva. 2006; 11 (1): 131-44.
17. Lakshmi SV, Srilatha A, Satyanarayana D, Reddy LS, Chalapathi SB, Meenakshi S. Oral health knowledge among a cohort of pregnant women in south India: A questionnaire survey. J Family Med Prim Care. 2020 Jun; 9 (6): 3015-9.
18. Kim EG, Park SK, Nho JH. Factors Related to Maternal Oral Health Status: Focus on Pregnant and Breastfeeding Women. Healthcare (Basel). 2021 Jun; 9 (6): 708.
19. Assimi S, Tajmouti R, Ennibi OK. Hygiène bucco-dentaire d'enfants scolarisés marocains et de leurs mères [Oral hygiene in Moroccan school children and their mothers]. Sante Publique. 2016 Mar-Apr; 28 (2): 245-50. [French]
20. Adeniyi A, Donnelly L, Janssen P, Jevitt C, Kardeh B, von Bergmann H, Brondani M. Pregnant women's perspectives on integrating preventive oral health in prenatal care. BMC Pregnancy Childbirth. 2021 Apr; 21 (1): 271.
21. Corchuelo-Ojeda J, González Pérez GJ, Casas-Arcila A. Factors Associated With Self-Perception in Oral Health of Pregnant Women. Health Educ Behav. 2022; 49 (1): 29-37.
22. Kabali TM, Mumghamba EG. Knowledge of Periodontal Diseases, Oral Hygiene Practices, and Self-Reported Periodontal Problems among Pregnant Women and Postnatal Mothers Attending Reproductive and Child Health Clinics in Rural Zambia. Int J Dent. 2018 Aug; 2018: 9782092.
23. Young-Wolff KC, Sarovar V, Alexeeff SE, Adams SR, Tucker LY, Conway A, et al. Trends and correlates of self-reported alcohol and nicotine use among women before and during pregnancy, 2009-2017. Drug Alcohol Depend. 2020 Sep; 214: 108168.
24. Llena C, Nakdali T, Sanz JL, Forner L. Oral Health Knowledge and Related Factors among Pregnant Women Attending to a Primary Care Center in Spain. Int J Environ Res Public Health. 2019 Dec; 16 (24): 5049.
Authors' contributionNapp N and Rigo L: Conceptualization, Data curation, Writing – original draft, Writing – review & editing, Visualization, Investigation, Validation, Formal analysis, Methodology, Supervision, Resources, Project administration. Alievi M and Belarmino RM: Conceptualization, Writing – review & editing, Visualization, Investigation, Validation, Methodology, Supervision, Resources. All authors approved the final version of the article and declare no conflicts of the interest.
Data availabilityAll datasets supporting the result of this study are included in the article.
Received on October 23, 2025
Final version presented on December 29, 2025
Approved on January 7, 2026
Associated Editor: Melania Amorim


 ; Marina Alievi2
; Marina Alievi2