ABSTRACT
OBJECTIVES: to analyze the effectiveness of acupuncture and laser therapy, either alone or in combination, in supporting and promoting breastfeeding, including their effects on pain reduction and wound healing.
METHODS: a systematic review was conducted using the PubMed, LILACS, IBECS, and BDENF databases through the Virtual Health Library (VHL), as well as SciELO. Search descriptors were guided by the PRISMA methodology. Studies evaluating acupuncture and/or low-level laser therapy in the context of breastfeeding support were included.
RESULTS: The reviewed studies assessed outcomes such as the reduction of breast pain associated with inflammatory symptoms, breast engorgement, milk production, and exclusive breastfeeding rates. Acupuncture was evaluated using different techniques, including needle acupuncture, Gua Sha, and Tuina. Low-Level Laser Therapy (LLLT) led to pain reduction in two clinical trials. However, one study found no difference between laser therapy and the control group regarding pain reduction in women with nipple trauma after a single local application.
CONCLUSIONS: the findings of this review indicate limited and heterogeneous evidence regarding breast pain reduction and breastfeeding support. Current evidence relies on a small number of clinical trials with small sample sizes, heterogeneous interventions, and distinct protocols, which precludes robust inferences or clinical recommendations. Further studies with rigorous methodological designs and standardized interventions are essential to clarify the role of these therapies in the clinical breastfeeding practice.
Keywords:
Breastfeeding, Mastodynia, Systematic review, Acupuncture, Low-level Laser therapy baixa intensidade
RESUMO
OBJETIVOS: analisar a efetividade da acupuntura e da laserterapia, associadas ou não, no suporte e apoio à amamentação, incluindo seus efeitos na dor e cicatrização.
MÉTODOS: foi realizada uma revisão sistemática nas bases Pubmed, LILACS, IBECS e BDENF, através da Biblioteca Virtual em Saúde (BVS), e Scielo utilizando descritores orientados pela metodologia Prisma, sendo incluídos artigos que avaliaram a acupuntura e/ou terapia de luz de baixa intensidade no suporte à amamentação.
RESULTADOS: os artigos encontrados tiveram como desfechos a diminuição da dor mamária em sintomas inflamatórios, ingurgitamento mamário, produção de leite e taxa de aleitamento materno exclusivo. A acupuntura foi analisada na aplicação por agulhas, Gua-sha e Tuiná. O uso da Laserterapia de Baixa Intensidade Focal (LLLT) obteve redução da dor em dois ensaios clínicos. Um estudo não encontrou diferença entre laserterapia e grupo controle na redução de dor em mulheres com lesões mamilares após única aplicação local.
CONCLUSÕES: os resultados desta revisão indicam evidência limitada e heterogênea de redução da dor mamária e para o apoio à amamentação. Esses achados embasam-se em poucos ensaios clínicos, com amostras reduzidas, intervenções e protocolos distintos, o que impede, por sua vez, inferências robustas ou recomendações clínicas. Estudos adicionais, com expresso rigor metodológico e padronização das intervenções, são cruciais para com o esclarecimento do papel dessas terapias no contexto da amamentação.
Palavras-chave:
Aleitamento materno, Mastodinia, Revisão sistemática, Acupuntura, Terapia com luz de baixa intensidade
IntroductionBreastfeeding and its related problems have been widely addressed in public policies and academic literature over the years; however, gaps in research persist, and early weaning remains a reality in Brazil.
1 Public policies and the various promotional initiatives over recent decades have contributed to a significant increase of exclusive breastfeeding (EBF) prevalence among infants under six months of age, which from 2.9% in 1986 to 37.1% in 2006. This trend plateaued in 2013 (36.6%), a concerning stabilization that underscores the need to review and develop new strategies for fostering EBF.
2Studies with different methodologies point to various risk factors associated with breastfeeding, including smoking, mode of delivery, maternal educational attainment, a lack of breastfeeding counseling, and the absence of skin-to-skin contact between mother and newborn. Furthermore, clinical conditions such as breast engorgement, flat or inverted nipples, abrasions, and erythema also represent significant risk factors for breastfeeding difficulties and early weaning.
3,4,5 The most frequent problems associated with breastfeeding and early weaning relate to difficulties with the correct breastfeeding techniques, specifically regarding the baby positioning at the breast and incomplete breast emptying. Improper breastfeeding techniques and positions contribute to increased trauma, abrasions, lesions, pain and nipple infections, as well as breast engorgement, clogged ducts, and mastitis.
6 During the first days, it is essential for the postpartum woman receives technical and emotional support to ensure satisfactory breastfeeding; therefore, counseling by a qualified professional during the immediate puerperium is crucial.
7Maternal counseling consists of an effective dialogue between health professional mothers concerning breastfeeding, providing support for management and addressing concerns. This counseling promotes breastfeeding starting in the prenatal period, which serves as an excellent opportunity to motivate women to breastfeed.
8 In addition to maternal counseling to support EBF, new interventions and technologies have been incorporated over time into the
Sistema Único de Saúde (SUS) (Brazilian Public Health System). Initiatives such as the Baby-Friendly Hospital Initiative (BHFI), along with the promotion of best practices in childbirth and perinatal care, have contributed to improving the support provided to women for successful breastfeeding.
7Technologies such as acupuncture and low-level laser therapy are seldom discussed and incorporated within SUS; however, a few studies have already pointed to potential benefits regarding the effectiveness of these practices in improving trauma and pain, as well as in supporting breastfeeding.
9-12Acupuncture is defined as the insertion of needles (primarily) into specific points along energy channels or meridians to balance the body; it is one of the techniques used in Traditional Chinese Medicine (TCM). Complementing acupuncture, TCM uses techniques such as tuina, gua-sha, cupping therapy, and moxibustion, which are also based on meridians and acupuncture points, distinguishing them from herbal medicine and other therapeutic strategies within Chinese medicine.
13 Acupuncture assists in general pain management, and has demonstrated benefits on breastfeeding.
14,15 TCM and acupuncture have been recognized by the SUS under the National Policy of Integrative and Complementary Practices as early as 2006, with their implementation, service expansion and effectiveness research serving as key objectives for the development of these practices in the country.
16The low-level laser therapy (LLLT) is not classified as an integrative practice; however, it may be used in conjunction with acupuncture. Low-level laser induces the healing process by acting on cellular metabolism, increasing granulation tissue, and reducing inflammatory mediators, thereby promoting collagen synthesis, tissue growth factors, revascularization, and pain relief.
9,17 The aim of this systematic review is to identify studies assessing the effectiveness of acupuncture and laser therapy, whether combined or not, in breastfeeding support, with the objective of understanding the effects of low-level laser therapy and acupuncture on breast pain and other breastfeeding-related challenges.
MethodsA systematic review was conducted to analyze publications investigating the use of acupuncture and/or low-level light therapy, either as standalone interventions or in combination, and their effectiveness in relieving breast pain and breastfeeding. Studies were included if they involved women practicing exclusive or mixed breastfeeding, with the intention to exclusively breastfeed, who presented with breast pain or other breastfeeding-related issues. The outcomes of interest were breast pain reduction and adherence to exclusive breastfeeding (EBF). The review followed the PRISMA 2020
18 recommendations and is derived from the master's thesis of one of the authors, developed within the Graduate Program in Collective Health of the Federal University of Paraíba. The review protocol is registered on the OSF platform (10.17605/OSF.IO/T89BY).
Research question:"
In lactating women with breast pain or breastfeeding-related issues, does the application of acupuncture and/or low-level laser therapy (either alone or in combination), compared to standard care, placebo, or no intervention, improve exclusive breastfeeding adherence and reduce pain?"
PICO structure:• P (Population): Lactating women with breast pain or breastfeeding-related issues.
• I (Intervention): Acupuncture and/or LLLT (either alone or in combination).
• C (Comparison): Standard care, placebo, or no intervention.
• O (Outcomes): Adherence to exclusive breastfeeding and pain reduction.
The included controlled clinical trials were those investigating the application of acupuncture and/or low-level light therapy as breastfeeding-supporting strategies for lactating women with breast pain or other breastfeeding-related issues, aiming at maintaining or returning to exclusive breastfeeding (EBF) in full-term infants. Complementary techniques were included if they were based on the acupuncture meridian system, such as acupuncture, tuina, gua-sha, and acupressure. Observational studies (cohorts, case series, or case reports), theses or dissertations without primary data, studies lacking a control group, and TCM interventions that did not utilize the meridian system (e.g., herbal medicine or diet therapy were excluded. Additionally, studies were excluded if essential methodological data could not be obtained (e.g., lack of description of the randomization process, absence of statistical analysis, or incomplete data for the outcomes of interest).
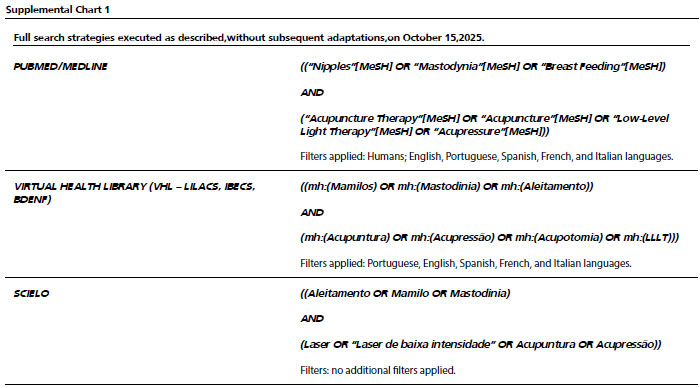
Bibliographic searches were performed on October 15, 2025, in the PubMed/MEDLINE, LILACS, IBECS and BDENF databases, via the Virtual Health Library (VHL), as well as in the SciELO database. The complete search strategies – like Boolean operators, indexing fields and parenthesis – are presented in Supplemental Chart 1 (Chart S1), allowing for the full reproduction of the search process. No restrictions were applied regarding the year of publication. Studies published in Portuguese, English, Spanish, Italian, and French were considered. When available on the platforms, human studies were prioritized. Study selection began with the manual identification and removal of duplicates by comparing titles, authors, publication years, and journals. Following deduplication, unique records were screened based on titles and abstracts. Study selection was conducted independently by three reviewers, based on predefined inclusion and exclusion criteria. The selection process occurred in two stages: (1
) Title and abstract screening and
(2) full-text review of potentially eligible articles. The number of records identified, duplicated, excluded, and included is shown in the PRISMA flowchart (Figure 1), in accordance with the methodological description.
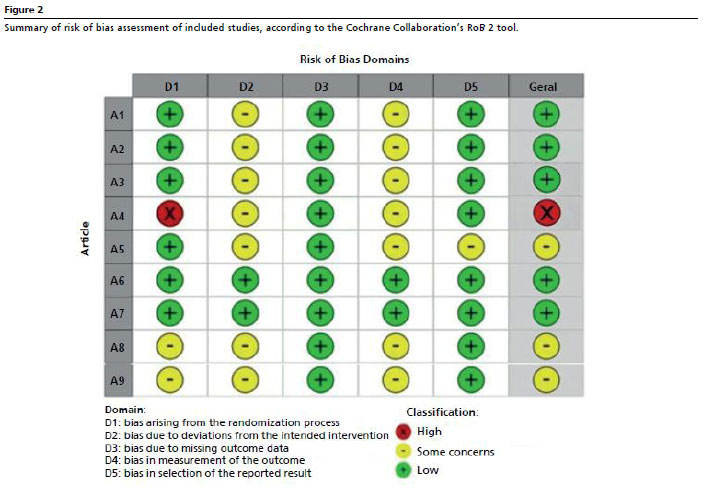
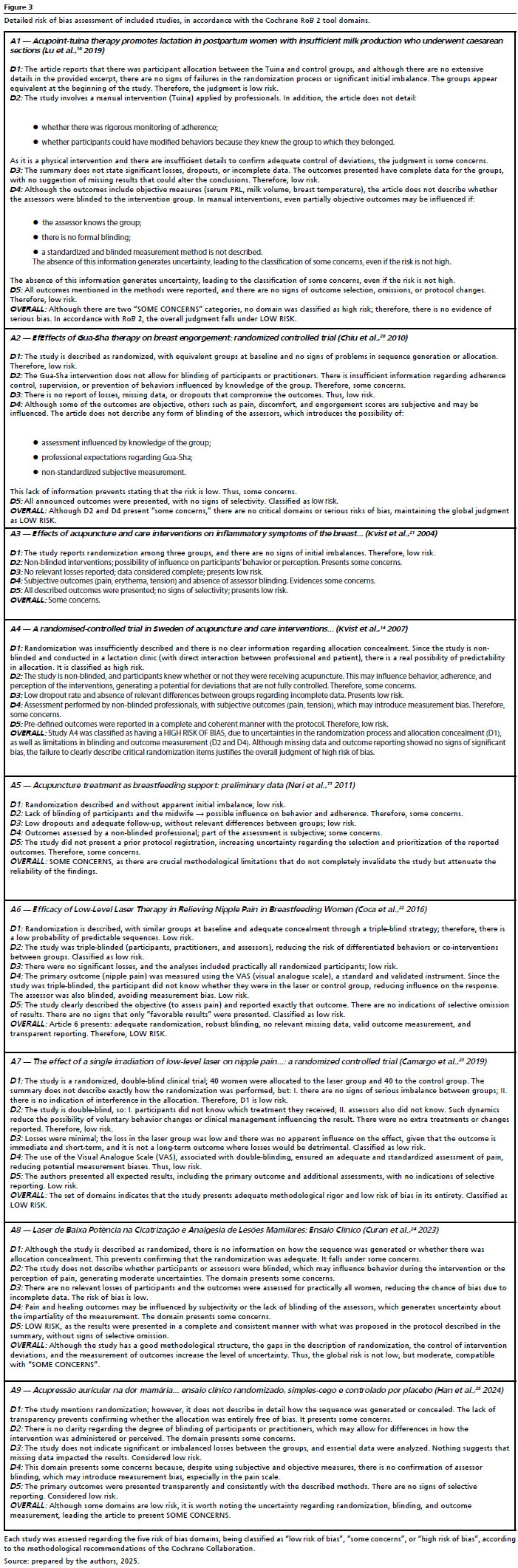
Furthermore, the risk of bias assessment of included studies was conducted independently by three reviewers using the Cochrane Collaboration's Risk of Bias 2 (RoB 2) tool for randomized clinical trials (Figure 2). Any disagreements among the reviewers were resolved by consensus. The RoB 2 tool assesses five domains:
1) Randomization process, (2) Deviations from intended interventions, (3) Missing outcome data, (4) Measurement of the outcome, and (5) Selection of the reported results (Figure 2).
Each domain was classified as low risk of bias, some concerns, or high risk of bias, according to RoB 2 guidelines.
19 The overall risk of bias judgement for each study was determined hierarchically, strictly adhering to the tool's recommendations: studies with at least one domain classified as high risk of bias were judged to have an overall high risk of bias; studies with no domains at high risk, but at least one domain classified as some concerns were judged as having some concerns; and only studies with all domains classified as low risk of bias were considered to have a low risk of bias. The detailed results of this analysis, including the justification for each judgement, are presented in Supplemental Chart 1, ensuring the transparency and reproducibility in the systematic review.
ResultsThe systematic review search yielded a total of 23 articles. After removing duplicates, 21 studies remained for title and abstract screening, leading to the exclusion of 12 studies for not meeting the inclusion criteria. Thus, the final selection comprised nine articles. Although the included studies presented significant results regarding the use of acupuncture and laser therapy in the context of breastfeeding, significant heterogeneity among methodological designs, sample sizes, and assessment tools. This variability limits the strength of evidence and hinders direct comparison between findings. 12 studies were excluded for the following reasons: they did not address acupuncture meridians and points or laser therapy; they did not involve the target population; or they presented methodological issues (
one study used secondary data without detailing sampling process, and another study had an inadequate sample with potential bias) (Figure 1). There were no disagreements among reviewers during the selection process. Study selection was conducted in two stages:
title and abstract screening, followed by
full-text review of potentially eligible articles. The process was conducted independently by the reviewers, and any disagreements were resolved by consensus, without the use of reference management software or automated tools.
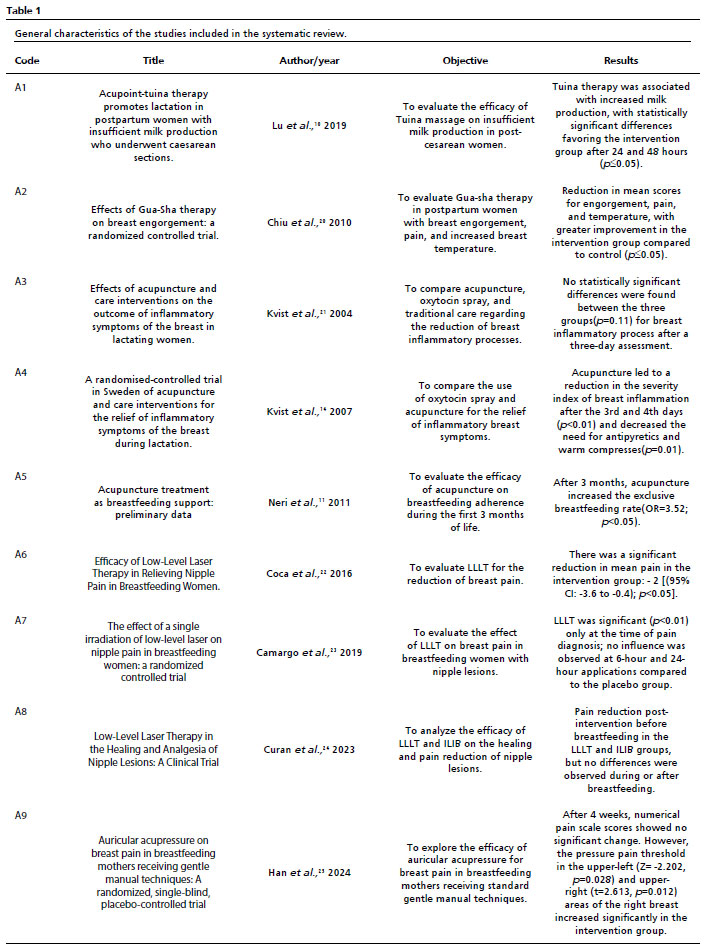
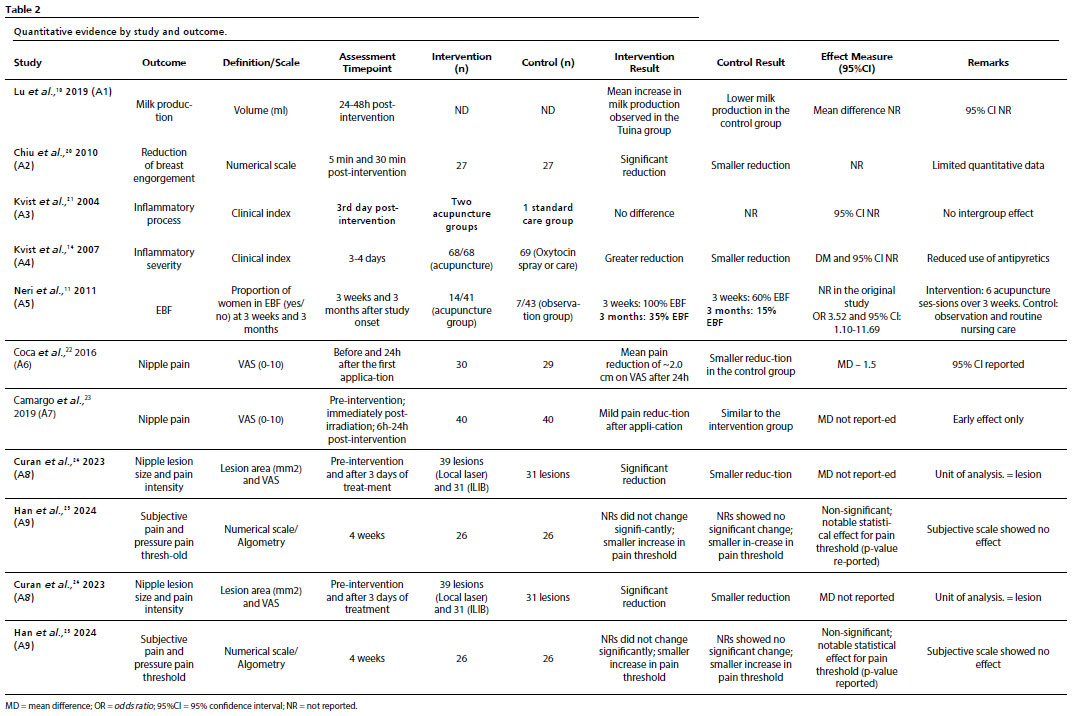
A total of 756 women were evaluated, with sample sizes ranging from 52 to 205 participants. Methodological designs, interventions, assessed outcomes, and follow-up periods were heterogeneous. No study directly compared acupuncture and laser therapy, nor did any assess the combined effect of these interventions. The analyzed outcomes included breast pain reduction, improvement of inflammatory symptoms, breast engorgement, nipple lesion healing, milk production, and adherence to exclusive breastfeeding. Table 1 summarizes the general representation of the characteristics of the included studies, while Table 2 systematically presents quantitative data by study and outcome, including the number of participants per group, outcome definition and scales, measurement timing, group statistics, and effect measures with their respective 95% confidence intervals, when available.
Study A1
10 analyzed 80 women with breast pain, equally distributed between the control and intervention groups. Both groups received standard hospital care, and the intervention group also underwent tuina massage for two consecutive days, starting 48 hours postpartum. Milk production was monitored through direct and indirect measures, including the volume produced. Higher mean milk production was observed 24 and 48 hours after the intervention in the tuina massage group compared to the control group, whereas no significant difference existed between the groups at baseline.
In study A2,
20 54 postpartum women with breast engorgement were allocated into control and intervention groups; the former received conventional treatment, while the latter received conventional treatment combined with gua-sha therapy. Engorgement, pain, and breast and body temperature scores were assessed. The intervention group showed a greater mean reduction in these scores throughout the follow-up period compared to the control group.
The publication A3
21 analyzed 88 lactating women with inflammatory breast symptoms who sought care at breastfeeding clinics. Participants were randomized into three groups: the first received conventional treatment combined with oxytocin spray; the second received acupuncture at the HT3 and GB21 points; and the third received acupuncture at the HT3, GB21, and SP6 points. No significant differences were observed between groups regarding the severity index of the inflammatory process, breastfeeding satisfaction, or response over time.
In the clinical trial A4
14, five lactating women reporting inflammatory breast processes were randomly assigned to three groups; all participants received standard treatment, supplemented with either oxytocin spray or acupuncture using different point combinations. A greater reduction in the severity index of the inflammatory process was observed in the acupuncture groups, as well as a reduced need for antipyretics and warm compresses, compared to the group using oxytocin spray alone.
The study A5
11 evaluated 84 lactating women, with 43 in the control group and 41 in the intervention group. The intervention group received acupuncture sessions twice a week for three weeks. The analysis was based on a semi-structured questionnaire administered during the study, after the third week of intervention and at the infant's three-month follow-up. The newborn's growth rate, the need for infant formula supplementation, and a subjective assessment of breastfeeding satisfaction were explored. In this study, the proportion of women adhering to breastfeeding was higher in the acupuncture group at both the three-week and three-month marks; raw data by group and the corresponding effect measures are presented in Table 2.
In the publication A6,
22 54 women were analyzed, with 30 in the LLLT intervention group and 29 in the placebo group. After multiple applications, a greater mean reduction in nipple pain was observed in the group receiving LLLT, as assessed by the Visual Analog Scale (VAS).
Study A7
23 evaluated breast pain in 80 women, with 40 assigned to the LLLT intervention group and 40 to the placebo group. Pain was monitored using the Visual Analog Scale (VAS) at three time points: at diagnosis, and at 6 and 24 hours after the initial application. Early LLLT application was associated with a greater reduction in pain at the time of diagnosis, while no consistent differences were observed during subsequent assessment periods.
Study A8
24 analyzed 105 nipple lesions in 54 lactating women who reported breastfeeding-related pain. The lesions were randomized into three groups: a control group, a local LLLT group, and an intravascular laser blood irradiation (ILIB) group—ILIB being a specific modality of low-level laser therapy. A reduction in both lesion size and pain before breastfeeding was observed in the intervention groups. However, since the unit of analysis was the lesion rather than the patient, and no adjustment for intra-subject dependence was performed, these findings should be interpreted with caution due to the risk of inflated statistical significance.
Study A9
25 evaluated the effectiveness of auricular acupressure on breast pain in 52 lactating women, all of whom also received a standard gentle manual technique. Participants were randomized into an intervention group, receiving auricular acupressure at specific points related to breast pain and lactation, and a placebo control group, which received stimulation at non-specific points. Pain intensity was assessed using a Numerical Rating Scale (NRS) and pressure algometry before and after the four-week intervention. No significant reduction was found in subjective pain scores on the NRS. However, a statistically significant increase in the pressure pain threshold in the upper areas of the right breast was observed in the intervention group. Auricular acupressure showed potential as a complementary nursing intervention, although further research is needed to define the optimal frequency and duration of the treatment, especially for women with more severe pain, and to evaluate the sustainability of long-term effects.
Risk of bias assessment of included studiesThe risk of bias assessment revealed methodological variability among the included studies (Figures 2 and 3). Five studies were classified as having an overall low risk of bias, as they demonstrated adequate randomization, satisfactory control of intervention deviations, complete data, and appropriate outcome measurement.
Three studies were classified as having some concerns, primarily due to the lack of blinding of participants and outcome assessors—a common limitation in manual interventions such as acupuncture, gua sha, and tuina—and an incomplete description of the randomization process.
One study was judged as having a high risk of bias due to substantial uncertainties regarding the randomization process, lack of allocation concealment, and the assessment of subjective outcomes by non-blinded assessors.
Overall, the domains most frequently associated with methodological concerns were those related to deviations from intended interventions and measurement of the outcome, which reduces confidence in the effect estimates presented.
DiscussionThe findings of this systematic review can be grouped into three major categories: the use of manual acupuncture; the application of LLLT or ILIB for breast pain or lesions; and the use of other techniques derived from the acupuncture meridian system. In all cases, the available evidence is limited and marked by methodological heterogeneity, which warrants caution when interpreting the findings.
LLLT showed divergent results among the included studies. One study observed no significant difference after a single application,
23 while two studies reported a reduction in pain associated with laser therapy.
22,24 However, the trials were limited by small sample sizes, varying protocols, and short follow-up periods, which restricts the robustness of the conclusions and hinders direct comparison between results.
Acupuncture was employed through various modalities, including manual acupuncture, tuina, and gua sha, and was compared to control groups or other interventions, such as oxytocin spray. Gua sha demonstrated pain reduction compared to a control group,
20 while tuina was associated with increased milk production in another study.
10 In a separate trial, manual acupuncture was associated with improved rates of exclusive breastfeeding.
11 Conversely, one study found no significant differences between the use of oxytocin spray and acupuncture protocols.
21 The variability in techniques, point selection, and evaluated outcomes contributes to the observed heterogeneity and limits the generalizability of these findings.
Regarding LLLT and ILIB, the review identified three studies, two of which evaluated pain reduction following laser therapy, notwithstanding methodological differences. In one study, pain reduction was more evident after the second irradiation session.
22 Another trial showed significant differences between LLLT/ILIB and the control group prior to breastfeeding, yet no significant difference was found when comparing these two interventions against each other.
24 However, the third study found no differences between a single LLLT session and the control group concerning pain reduction in women with nipple lesions.
23 Such heterogeneity limits comparisons between trials and reinforces the need for standardized protocols and larger sample sizes.
In one of the included studies (A8
24), the unit of analysis was the breast lesion rather than the individual participant. In this design, multiple lesions from the same woman may have been analyzed as independent observations, posing a risk of intra-subject dependence. Consequently, this approach violates the assumption of independence of observations and may result in an overestimation of statistical significance and an artificial narrowing of confidence intervals. The study did not report the use of statistical methods for cluster adjustment, such as hierarchical models or corrections for intraclass correlation. Thus, although the results indicate a reduction in pre-breastfeeding pain and lesion size in the intervention groups, the certainty of these findings was downgraded in this systematic review. Therefore, the observed effects must be interpreted with caution, as exploratory and hypothesis-generating, rather than as robust evidence of clinical efficacy.
Regarding the risk of bias, several studies exhibited critical limitations, particularly concerning the blinding of participants and personnel, which is inherently challenging in interventions such as acupuncture and massage. Only two publications implemented adequate blinding strategies. These methodological shortcomings, coupled with small sample sizes and the risk of selection bias, diminish the confidence in the reported effect estimates.
Breastfeeding, although extensively studied, remains a notable challenge in Brazil, with high rates of early weaning influenced significantly by nipple trauma and pain, among other factors related to breastfeeding management.
26 The outcome of maintaining exclusive breastfeeding showed a significant increase with the use of acupuncture in one of the studies.
11 It is noteworthy that relatively simple application strategies, such as tuina, gua sha, and other massage techniques,
10,20 could be integrated into postpartum care practices. However, these findings should be interpreted as hypotheses for future research; they do not yet support formal clinical recommendations or health technology adoption decisions.
Despite preliminary evidence of benefit observed in some studies, the available data is limited, heterogeneous, and based on a small number of clinical trials—many characterized by small sample sizes and some concerns regarding the risk of bias. Therefore, the results should be interpreted descriptively and do not support formal clinical recommendations. It is important to emphasize that the observed effects of LLLT and ILIB primarily relate to breast pain reduction and lesion healing, whereas the impacts on the maintenance of exclusive breastfeeding are indirect and based on a limited number of studies. Future clinical trials with greater methodological standardization and combined assessment of interventions are required to confirm these findings.
Final considerationsThis systematic review synthetized the available evidence regarding the use of acupuncture, low-level laser therapy (LLLT), and intravascular laser blood irradiation (ILIB) in the management of breast pain and nipple lesions, and breastfeeding-related outcomes. Overall, several studies reported positive effects from these interventions, particularly concerning pain relief and lesion healing. Furthermore, sporadic indications of a favorable impact were observed regarding milk production and the maintenance of exclusive breastfeeding (EBF).
However, the available studies are limited and marked by methodological heterogeneity, variability in intervention protocols, small sample sizes, and moderate to high risk of bias across a portion of the included studies. Moreover, specific limitations – such as the use of non-independent units of analysis in one study and the lack of adequate statistical adjustments – diminish the reliability of certain findings.
Therefore, the results obtained in this review do not support formal clinical recommendations, nor health technology adoption decisions. The findings should be interpreted cautiously and descriptively, being considered exploratory and hypothesis-generating. Further studies with more robust methodological designs, greater standardization of interventions, adequate sample sizes, and rigorous outcome assessments are essential to clarify the effectiveness of the aforementioned therapies within the context of breastfeeding.
References1. Faria NT, Ferreira RD. Prevalência do aleitamento materno exclusivo no Brasil e fatores associados ao desmame precoce. Rev Ibero Am Humanidades Cienc Educ. 2022; 8 (4): 474-84.
2. Boccolini CS, Boccolini PD, Monteiro FR, Venâncio SI, Giugliani ER. Breastfeeding indicators trends in Brazil for three decades. Rev Saúde Pública. 2017; 51: 108.
3. Barbosa GE, Silva VB, Pereira JM, Soares MS, Medeiros Filho RD, Pereira LB, et al. Dificuldades iniciais com a técnica da amamentação e fatores associados a problemas com a mama em puérperas. Rev Paul Pediatr. 2017; 35 (3): 265-72.
4. Barbosa GE, Pereira JM, Soares MS, Pereira LB, Pinho L, Caldeira AP. Initial difficulties with breastfeeding technique and the impact on duration of exclusive breastfeeding. Rev Bras Saúde Matern Infant. 2018; 18 (3): 517-26.
5. Cohen SS, Alexander DD, Krebs NF, Young BE, Cabana MD, Erdmann P, et al. Factors associated with breastfeeding initiation and continuation: a meta-analysis. J Pediatr. 2018; 203: 190-6.
6. Santiago LB, Santiago FG. Aleitamento materno: técnica, dificuldades e desafios. Residência Pediátrica [Internet]. 2014 [access in 2024 Jan 8]; 3 (3Supl.1): S23-S30. Available from:
https://residenciapediatrica.com.br/detalhes/115/aleitamento-materno--tecnica--dificuldades-edesafios7. World Health Organization (WHO). Guideline: protecting, promoting and supporting breastfeeding in facilities providing maternity and newborn services. Geneva: WHO; 2017 [access in 2024 Jan 8]. Available from:
https://apps.who.int/iris/handle/10665/2593868. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Saúde da criança: aleitamento materno e alimentação complementar. Brasília (DF): Ministério da Saúde; 2015. [access in 2024 Jan 8]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/saude_crianca_aleitamento_materno_cab23.pdf.
9. Andrade FD, Clark RM, Ferreira ML. Effects of low-level laser therapy on wound healing. Rev Col Bras Cir. 2014; 41 (2): 129-33.
10. Lu P, Ye ZQ, Qiu J, Wang XY, Zheng JJ. Acupoint-tuina therapy promotes lactation in postpartum women with insufficient milk production who underwent caesarean sections. Medicine. 2019; 98 (35): e16456.
11. Neri I, Allais G, Vaccaro V, Minniti S, Airola G, Schiapparelli P, et al. Acupuncture treatment as breastfeeding support: preliminary data. J Altern Complement Med. 2011; 17 (2): 133-7.
12. Nogueira DN, Curan FM, Cardelli AA, Ferrari RA, Tokushima T, Andraus RA. Low- level laser: cost of therapy fornipple trauma. Rev Bras Saúde Matern Infant. 2021; 21 (1): 151-9.
13. Ergil MC, Ergil KV. Medicina chinesa: guia ilustrado. 1st ed. Porto Alegre: Artmed; 2010.
14. Kvist LJ, Louise Hall-Lord M, Rydhstroem H, Wilde Larsson B. A randomised-controlled trial in Sweden of acupuncture and care interventions for the relief of inflammatory symptoms of the breast during lactation. Midwifery. 2007; 23 (2): 184-95.
15. Takiguchi RS, Fukuhara VS, Sauer JF, Assumpção A, Marques AP. Efeito da acupuntura na melhora da dor, sono e qualidade de vida em pacientes fibromiálgicos: estudo preliminar. Fisioter Pesq. 2008; 15 (3): 280-4.
16. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Política Nacional de Práticas Integrativas e Complementares no SUS: atitude de ampliação de acesso. Brasília (DF): Ministério da Saúde; 2015. [Internet]. [access in 2024 Jan 8]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/politica_nacional_praticas_integrativas_complementare s_2ed.pdf.
17. Lins RD, Dantas EM, Lucena KC, Catão MH, Granville-Garcia AF, Carvalho Neto LG. Efeitos bioestimulantes do laser de baixa potência no processo de reparo. An Bras Dermatol. 2010; 85 (6): 849-55.
18. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. A declaração PRISMA 2020: diretriz atualizada para relatar revisões sistemáticas. Rev Panam Salud Publica [Internet]. 2022 [acesso em 2024 jan 8]; 46: 1. Disponível em:
https://doi.org/10.26633/rpsp.2022.11219. Sterne JA, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019; 366: l48- 98.
20. Chiu JY, Gau ML, Kuo SY, Chang YH, Kuo SC, Tu HC. Effects of gua-sha therapy on breast engorgement. J Nurs Res. 2010; 18 (1): 1-10.
21. Kvist LJ, Wilde Larsson B, Hall-Lord ML, Rydhstroem H. Effects of acupuncture and care interventions on the outcome of inflammatory symptoms of the breast in lactating women. Int Nurs Rev. 2004; 51 (1): 56-64.
22. Coca KP, Marcacine KO, Gamba MA, Corrêa L, Aranha AC, Abrão AC. Efficacy of low-level laser therapy in relieving nipple pain in breastfeeding women: a triple-blind, randomized, controlled trial. Pain Manag Nurs. 2016; 17 (4): 281-9.
23. Camargo BT, Coca KP, Amir LH, Corrêa L, Aranha AC, Marcacine KO, et al. The effect of a single irradiation of low-level laser on nipple pain in breastfeeding women: a randomized controlled trial. Lasers Med Sci. 2019; 35 (1): 63-9.
24. Curan FMS, Ferrari RAP, Andraus RAC, Tokushima T, Guassú DNO, Rodrigues R, et al. Laser de baixa potência na cicatrização e analgesia de lesões mamilares: ensaio clínico. Enferm Em Foco. 2023; 14: 1-7.
25. Han S, Kim B, Park H. Auricular acupressure on breast pain among breastfeeding mothers receiving gentle hand techniques: a randomized, single-blind, sham-controlled trial. J Hum Lact. 2024; 40 (2): 248-58.
26. Alvarenga SC, Castro DS, Costa Leite FM, Gomes Brandão MA, Zandonade E, Caniçali Primo C. Fatores que influenciam o desmame precoce. Aquichan. 2017; 17 (1): 93-103.
Author's contribution:Lima DL: conceptualization, systematic review structuring, study selection, data analysis, and manuscript writing.
Soares RS: systematic review structuring, supervision of the writing process, review and study selection, risk of bias assessment, manuscript review.
Macedo PO, Freitas ES, Souza IG, Pedro IKF: peer review of study selection, interpretation of findings, manuscript review.
Araújo JSS: project coordination and supervision of the systematic review structuring, manuscript review.
All authors approved the final version of the article and declare no conflicts of interest.
Data availabilityAll data analyzed in this systematic review were extracted from previously published studies and are available in the searched databases.
Received on November 27, 2025
Final version presented on January 27, 2026
Approved on January 30, 2026
Associated Editor: Alex Sandro Souza


 ; Ricardo de Sousa Soares2
; Ricardo de Sousa Soares2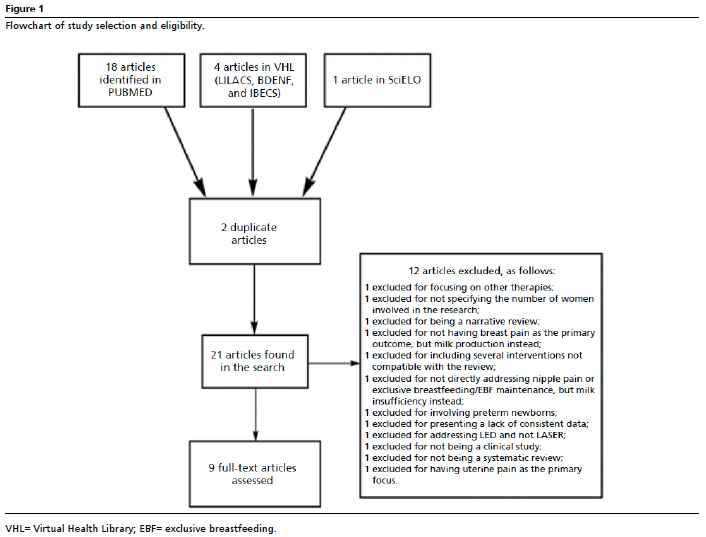






 Ler em português
Ler em português